

Retention of bimanual performance following hand arm bimanual intensive therapy in children with unilateral cerebral palsy: A six-month longitudinal study
- PMID: 39739775
- PMCID: PMC11687730
- DOI: 10.1371/journal.pone.0313018
Retention of bimanual performance following hand arm bimanual intensive therapy in children with unilateral cerebral palsy: A six-month longitudinal study
Abstract
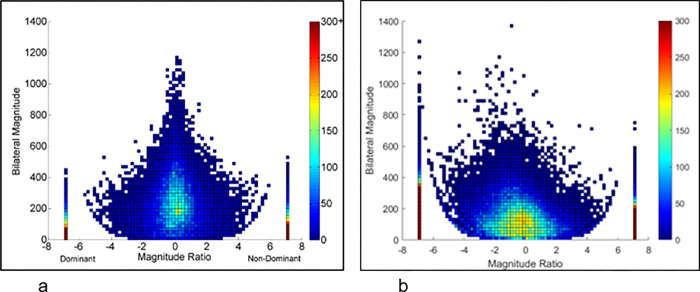
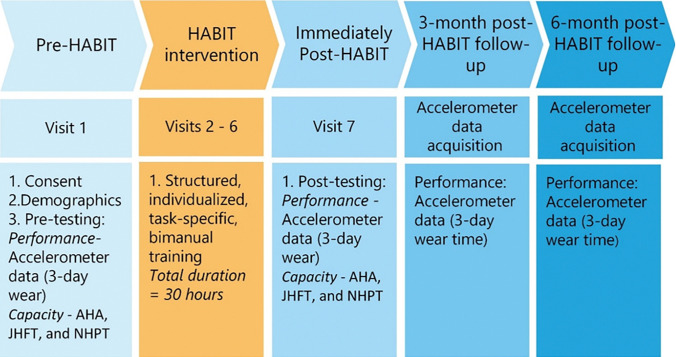
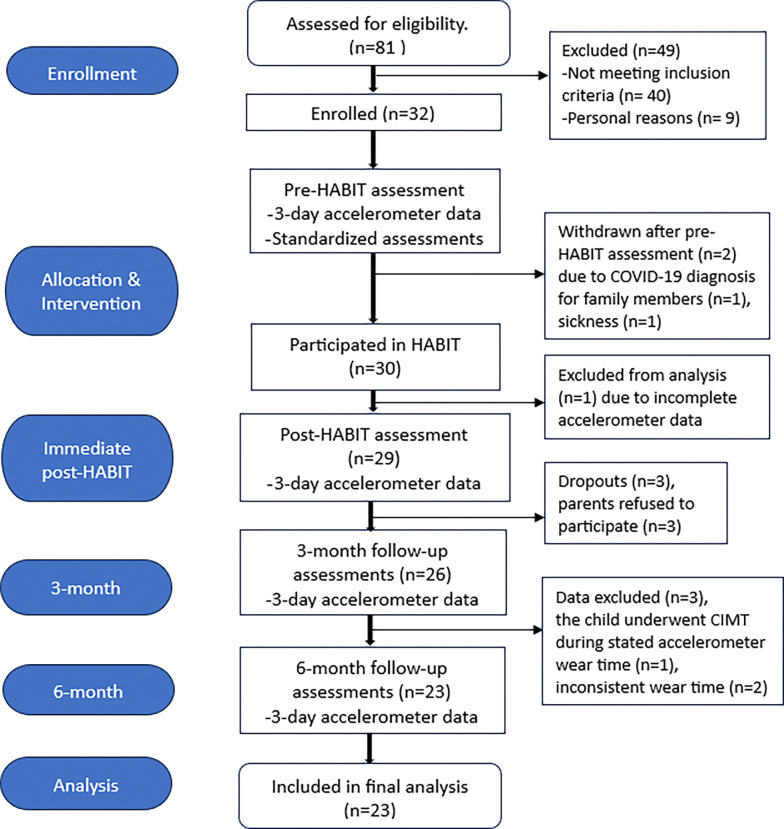
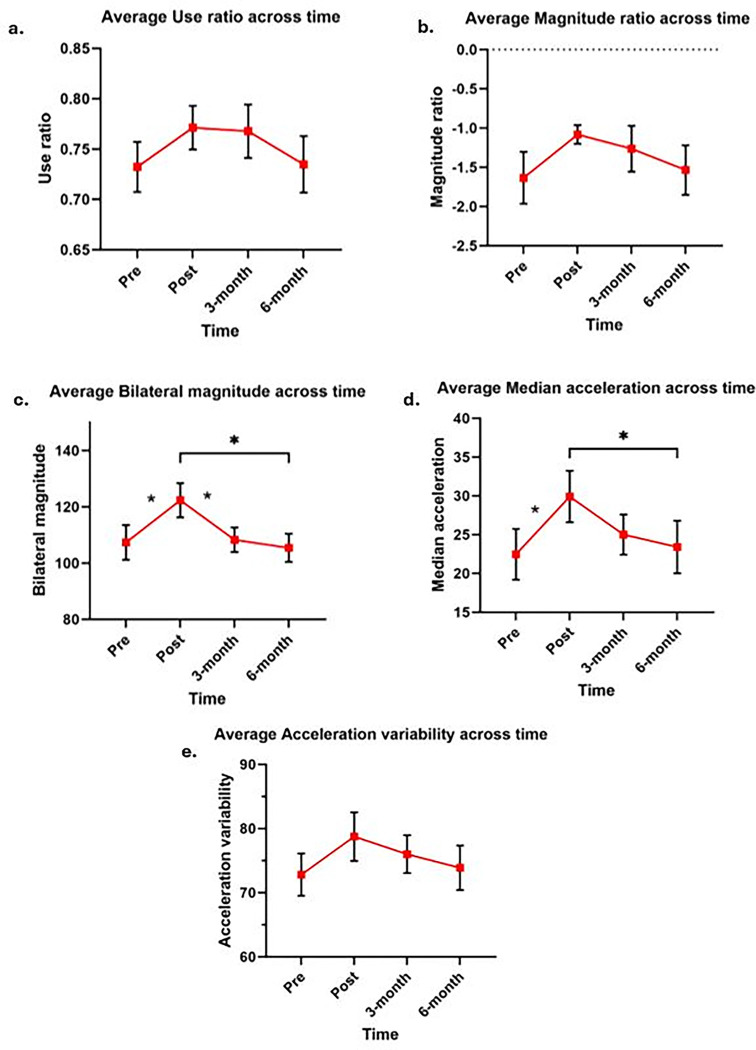
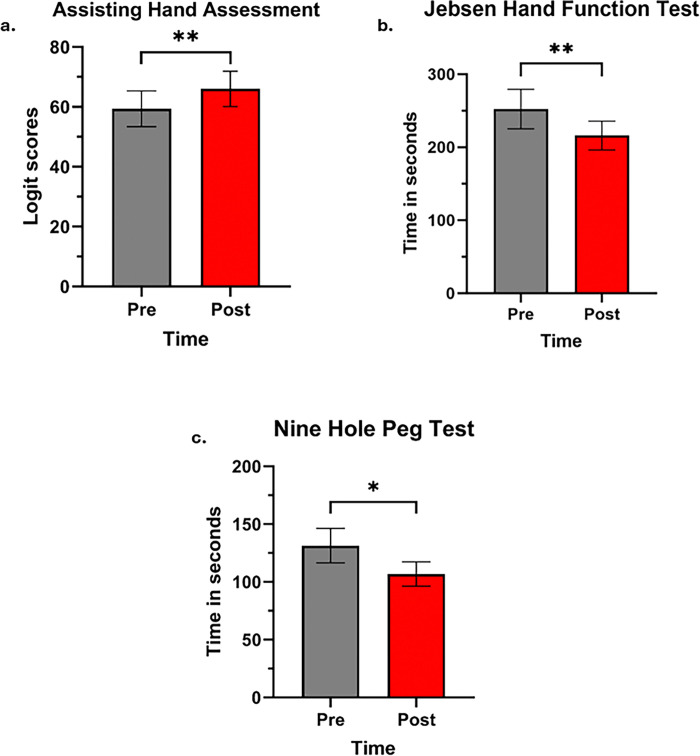
Hand-arm bimanual intensive therapy (HABIT) enhances upper extremity (UE) function and bimanual coordination in children with unilateral cerebral palsy (UCP). Previous studies assessed immediate improvements in UE function using clinical and self-reported measures, which may not accurately reflect real-world UE performance and their long-term retention effects. Therefore, this study aims to investigate the retention of real-world bimanual performance gains over time following HABIT in children with UCP. Thirty children with UCP, age 6-16 years underwent HABIT (6 hours/day for 5 days). Bimanual performance was assessed using GT9X Link accelerometers, worn on bilateral wrists for 3 days pre-, post-, 3-, and 6-month of HABIT. Accelerometer-derived variables-use ratio (UR), magnitude ratio (MR), bilateral magnitude (BM), median acceleration (MA), and acceleration variability (AV)-quantified bimanual performance during real-world activities. UE function was measured with standardized assessments. A mixed model analysis with repeated measures and paired t-tests analyzed the differences real-world bimanual performance and UE function respectively. There was a significant main effect of time in UR (F = 2.72, p = 0.05), BM (F = 4.36, p = 0.007), and MA (F = 3.68, p = 0.016). Post-hoc analysis (mean differences, 95% confidence interval [CI]) revealed improvements immediately post- compared to pre-HABIT in BM (14.99, 4.35-25.63) and MA (7.46, 2.55-12.36). However, subsequent assessments at 3- and 6-months displayed a regression in these gains, suggesting a lack of retention. A decline was observed at 3 months) and 6 months (BM; 16.94, 6.3-27.4, MA; 6.51, 1.61-11.41) in BM and MA compared to post-HABIT. UE capacity measures also showed improvements (p < 0.05) post-HABIT. Although HABIT initially may enhance performance of real-world bimanual tasks, its benefits diminish within six months, suggesting a need for repeating HABIT every 3-6 months to retain long-term improvements.
Copyright: © 2024 Gardas et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Kirby RS, Wingate MS, Van Naarden Braun K, Doernberg NS, Arneson CL, Benedict RE, et al. Prevalence and functioning of children with cerebral palsy in four areas of the United States in 2006: A report from the Autism and Developmental Disabilities Monitoring Network. Res Dev Disabil. 2011. Mar;32(2):462–9. doi: 10.1016/j.ridd.2010.12.042 - DOI - PubMed
-
- Rosenbaum P, Paneth N, Leviton A, Goldstein M, Bax M, Damiano D, et al. A report: the definition and classification of cerebral palsy April 2006. Dev Med Child Neurol Suppl. 2007. Feb;109:8–14. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
