

Exploring the associations of sleep bruxism and obstructive sleep apnea with migraine among patients with temporomandibular disorder: A polysomnographic study
- PMID: 39740030
- PMCID: PMC11794979
- DOI: 10.1111/head.14892
Exploring the associations of sleep bruxism and obstructive sleep apnea with migraine among patients with temporomandibular disorder: A polysomnographic study
Abstract
Background: Migraine is the most common disabling headache disorder in the world. Temporomandibular disorders (TMDs) are a group of conditions characterized by pain/dysfunction of masticatory muscles or their associated structures. There is a lack of studies concerning the association between sleep disorders such as sleep bruxism (SB), obstructive sleep apnea (OSA), migraine, and TMD, despite the increased prevalence of these conditions in TMD patients.
Objective: Our case-control study assesses the potential relationship among SB, OSA, and migraine using polysomnography (PSG) among the group with TMD.
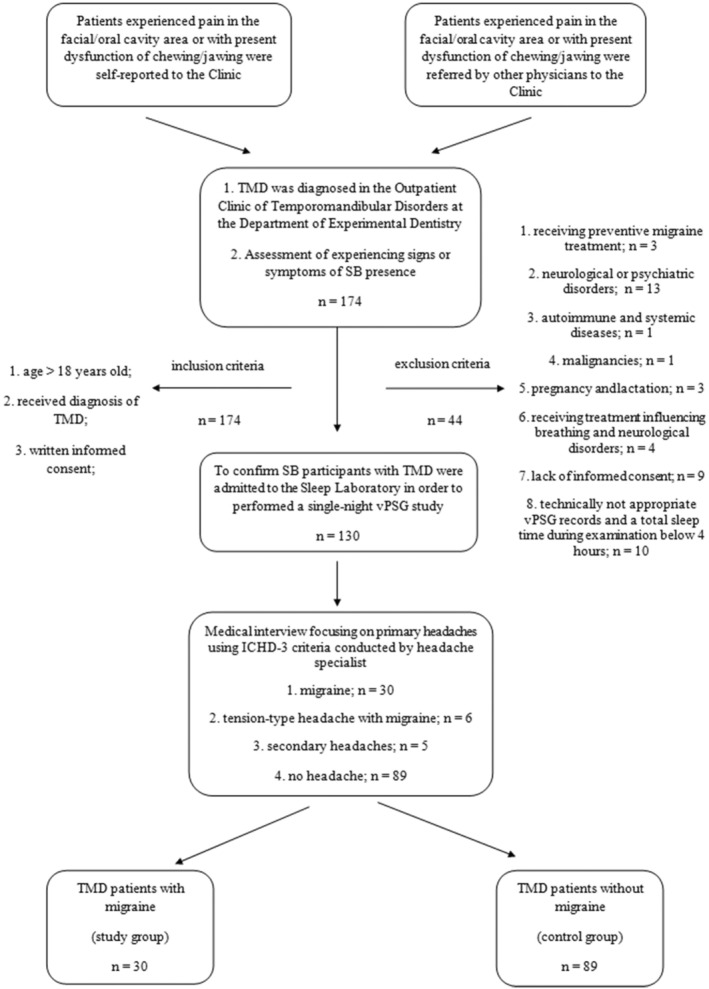
Methods: One hundred nineteen patients with TMD were recruited and hospitalized in the Department and Clinic of Internal Medicine, Occupational Diseases, Hypertension, and Clinical Oncology at Wroclaw Medical University. Their sleep parameters were assessed by PSG according to American Academy of Sleep Medicine guidelines. Migraine diagnosis was based on the third edition of the International Classification of Headache Disorders. The group of 30 patients with median age 35.0 years (interquartile range [IQR]: 26.0, 41.0) were diagnosed with migraine and this group consisted of 17 without aura (MwoA) and 13 with aura (MwA). Thirty patients with migraine were compared to 89 patients with TMD without migraine (controls) with median age 37.0 years (IQR: 26.0, 44.0).
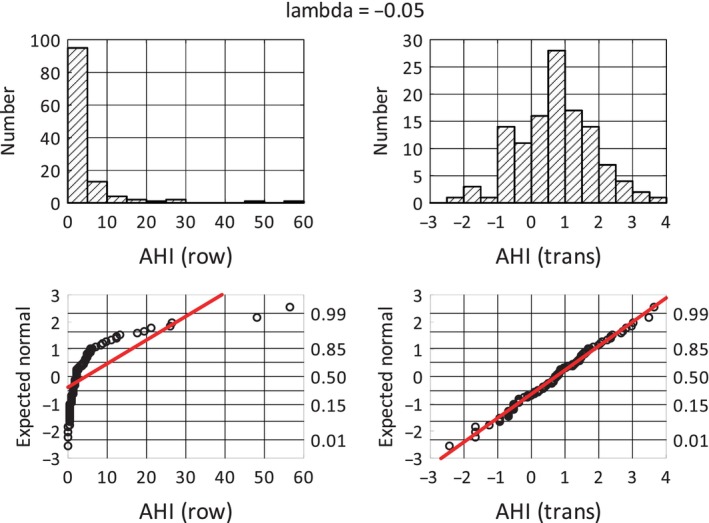
Results: Sleep bruxism was detected in 86% of the migraine group and 71.9% of control participants. The median bruxism episode index (BEI) among patients with migraine was 3.8 n/h (IQR: 2.7, 5.8) and 3.5 n/h (IQR: 1.8, 6.0) in the control group. SB and severe SB (respectively, BEI > 2 and BEI > 4) were not associated with migraine (odds ratio [OR] = 2.68, 95% confidence interval [CI]: 0.84-8.55, p = 0.095; OR = 0.98, 95% CI: 0.42-2.32, p = 0.966). However, mixed bruxism episodes were more frequent in the migraine group compared to study participants not experiencing migraine (median 0.7 n/h [IQR: 0.4, 1.6] vs. median 0.5 n/h [IQR: 0.2, 0.9], p = 0.044; OR = 1.96 with 95% CI: 1.16-3.32, p = 0.013). The median average duration of SB episodes in the migraine group was longer than in the controls (7.0 s [IQR: 5.5, 8.4] vs. 5.9 s [IQR: 5.1, 6.6], p = 0.005). The apnea-hypopnea index (AHI) value was not associated with migraine compared to controls (OR = 1.01, 95% CI: 0.96-1.06, p = 0.605), but MwoA had significantly increased AHI values compared to MwA (mean AHI = -0.1, standard deviation [SD] = 1.5 for MwA vs. mean AHI = 0.9 with SD = 1.3 for MwoA, p = 0.049).
Conclusion: Sleep bruxism may not be associated with migraine among patients with TMD; however, mixed bruxism episodes were more frequent in the migraine group. The increased duration of SB episodes in patients with migraine may suggest the common background of these conditions. OSA is also not associated with migraine; however, MwoA might increase the odds of OSA. There is a need to further explore sleep disturbances and migraine, especially in groups with their increased prevalence, such as patients with TMD.
Keywords: TMD; aura; bruxism episode index; migraine.
© 2024 The Author(s). Headache: The Journal of Head and Face Pain published by Wiley Periodicals LLC on behalf of American Headache Society.
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
