

Clinical and ultrasound characteristics in patients with sars-cov-2 pneumonia, associated with hospitalization prognosis. e-covid project
- PMID: 39741236
- PMCID: PMC11686988
- DOI: 10.1186/s12890-024-03439-2
Clinical and ultrasound characteristics in patients with sars-cov-2 pneumonia, associated with hospitalization prognosis. e-covid project
Abstract
Background: During the COVID-19 pandemia, the imaging test of choice to diagnose COVID-19 pneumonia as chest computed tomography (CT). However, access was limited in the hospital setting and patients treated in Primary Care (PC) could only access the chest x-ray as an imaging test. Several scientific articles that demonstrated the sensitivity of lung ultrasound, being superior to chest x-ray [Cleverley J et al., BMJ 370, 202013] and comparable to CT scan [Tung-Chen Y et al., Ultrasound Med Biol 46:2918-2926, 2020], promoted the incorporation of this technique in the assessment of COVID-19 patients in PC. [Pérez J et al., Arch. Bronconeumol 56:27-30, 2020; Gargani L et al., Eur Heart J Cardiovasc Imaging 21:941-8, 2020, Soldati G et al., J Ultrasound Med 39:1459, 2020] A prior study in our territory (Lleida, Spain) was designed to predict complications (hospital admission) of COVID-19 pneumonia in PC patients, being different patterns of Lung ultrasounds (LUS) risk factors for hospital admission. [Martínez Redondo J et al., Int J Environ Res Public Health 18:3481, 2021] The rationale for conducting this study lies in the urgent need to understand the determinants of severity and prognosis in COVID-19 patients with interstitial pneumonia, according to its lung ultrasound patterns. This research is crucial to provide a deeper understanding of how these pre-existing ultrasound patterns related to disease progression influence the medical treatment.
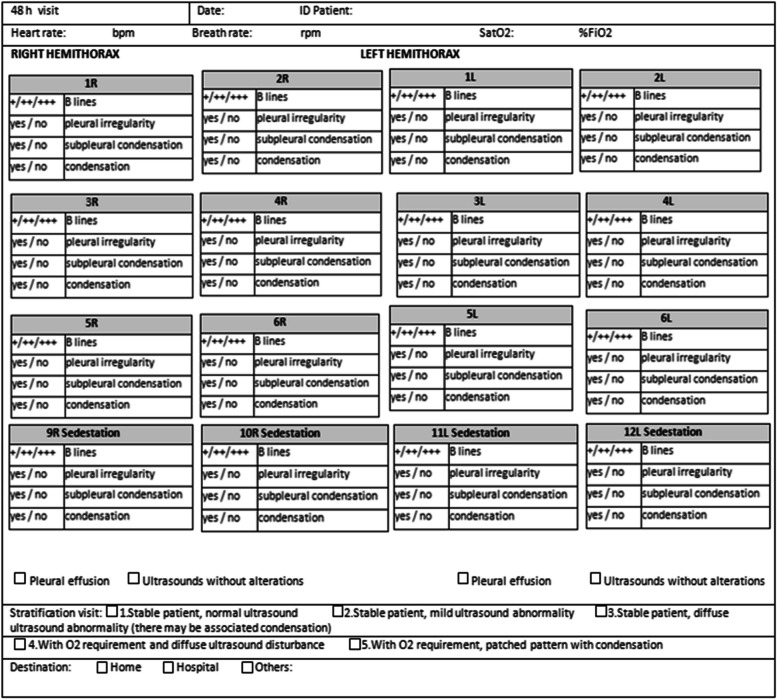
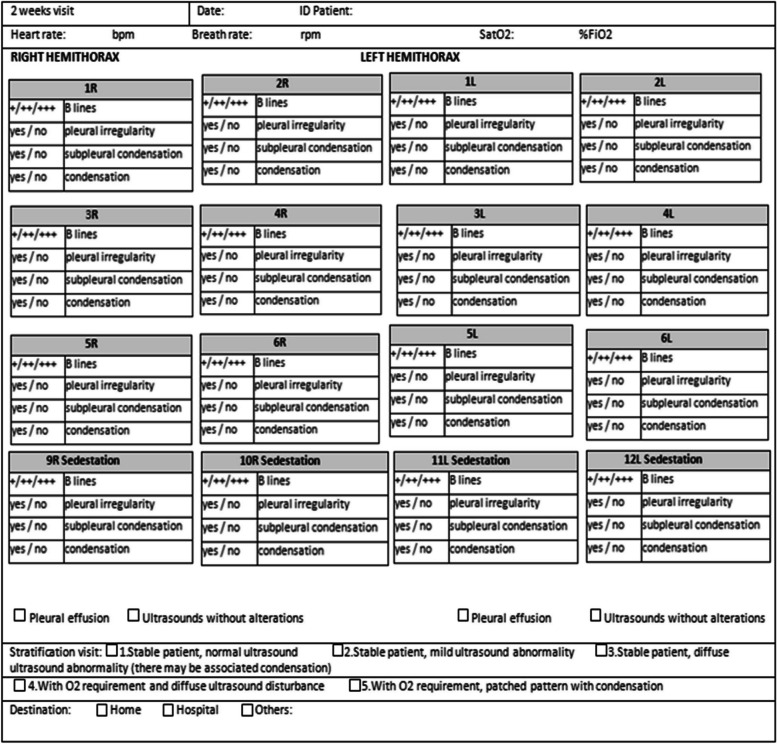
Methods: The objective of the study is to generate predictive models of lung ultrasound patterns for the prediction of lung areas characteristics associated with hospitalizations and admissions to the Intensive Care Unit (ICU) associated with COVID-19 disease, using ultrasound, sociodemographic and medical data obtained through the computerized medical history.
Results: A single relevant variable has been found for the prediction of hospitalization (number of total regions with potentially pathological presence of B lines) and one for the prediction of ICU admission (number of regions of the right lung with potentially pathological presence of B lines). In both cases it has been determined that the optimal point for classification was 2 or more lung affected areas. Those areas under the curve have been obtained with good predictive capacity and consistency in both cohorts.
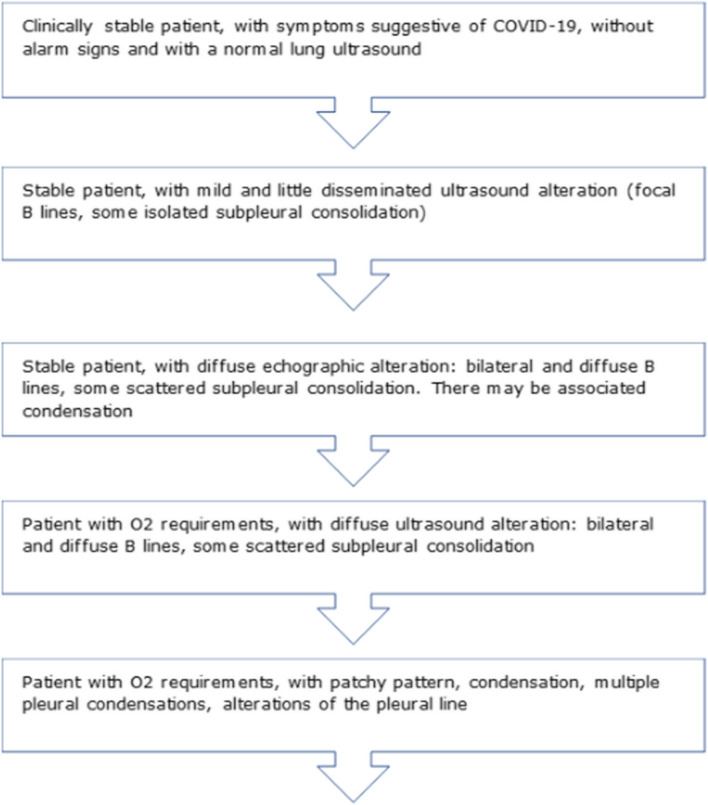
Conclusions: The results of this study will contribute to the determination of the ultrasound prognostic value based on the number of lung areas affected, the presence of pulmonary condensation or the irregularity of pleural effusion patterns in COVID-19 patients, being able to be extended to other lung viral infections with similar patterns.
Keywords: Hospitalization; Primary health care; Prognosis; SARS-CoV-2; Ultrasound.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study protocol and study methodology was approved by ethic committees by the Clinical Research Ethics Committee (CEIC) of the Primary Care Research Institute (IDIAP Jordi Gol). Registration CEIC 20/080-PCV. Once the project information sheet has been explained and delivered, written consent has been requested for participation in the study. Those patients who have started the already existing circuit for the diagnosis and follow-up of COVID-19 patients using ultrasound, prior to the start of the study, had been contacted by phone and their written consent has been requested. Informed consent was obtained from all subjects involved in the study. The collected variables had been treated anonymously and guaranteeing the confidentiality of the data, according to the provisions of Regulation (EU) 2016/679 of the European Parliament and the Council of April 27 on data protection (RGPD) and the organic law 3 /2018, of December 5, on the protection of personal data and the guarantee of digital rights. The database is in the hands of the IP and the research team in an Excel format and with password access. An anonymized database has been used for the analysis. This study was approved by the Ethical Committee of Institut d’Investigació en Atenció Primària Jordi Gol i Gurina (Barcelona, Spain) (registration number p20/138). Consent for publication: Not Applicable. Competing interests: The authors declare no competing interests.
Figures





References
-
- World Health Organization. Novel Coronavirus (2019-nCoV), Situational report. WHO Bull [Internet]. 2020;(10):1–7. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/2...
-
- Ap C. Consulta telefònica en temps de la covid-19 . Experiència en un centre de salut urbà La covid-19 posa en evidència la urgència d ’ espais dignes als centres d ’ atenció primària de Barcelona. Butlletí camfic. :1–60.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
