

Diabetes Mellitus and Cardiovascular Disease: Exploring Epidemiology, Pathophysiology, and Treatment Strategies
- PMID: 39742220
- PMCID: PMC11683709
- DOI: 10.31083/j.rcm2512436
Diabetes Mellitus and Cardiovascular Disease: Exploring Epidemiology, Pathophysiology, and Treatment Strategies
Abstract
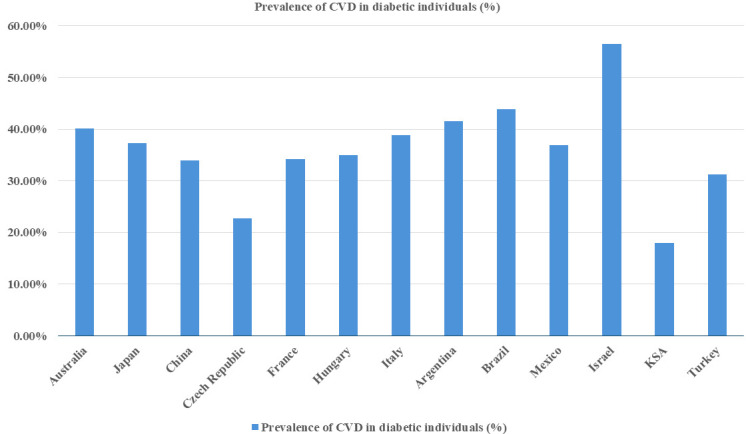
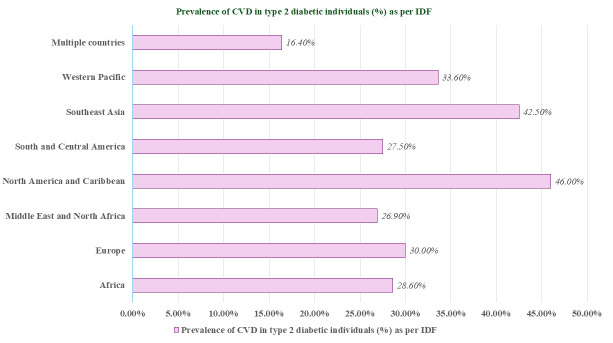
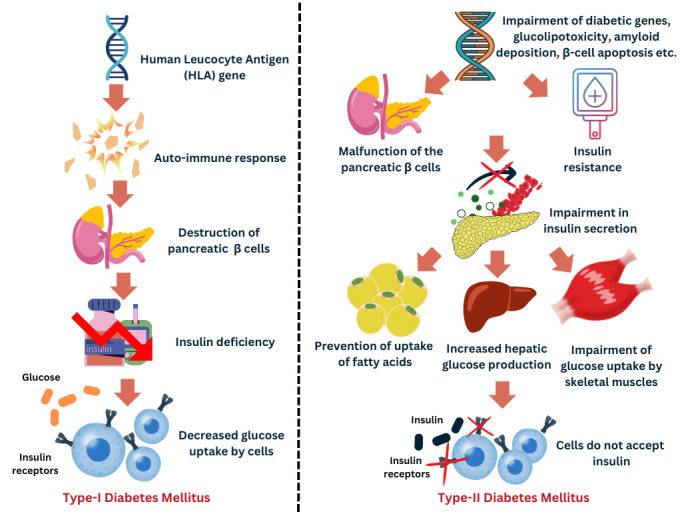
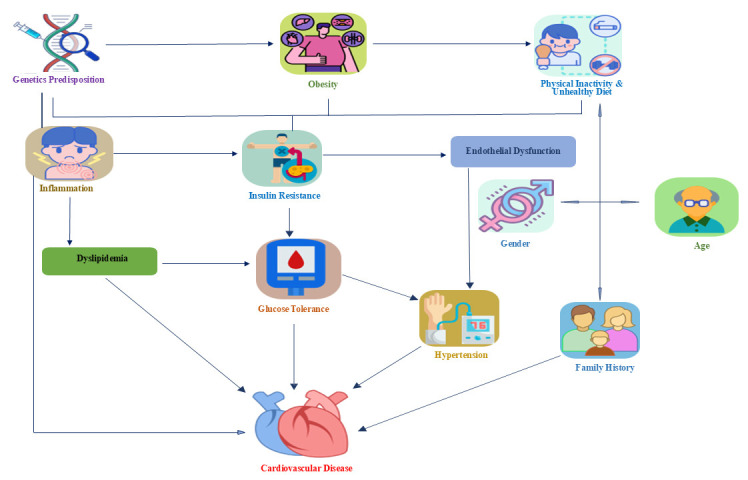
Diabetes mellitus (DM) affects 537 million people as of 2021, and is projected to rise to 783 million by 2045. This positions DM as the ninth leading cause of death globally. Among DM patients, cardiovascular disease (CVD) is the primary cause of morbidity and mortality. Notably, the prevalence rates of CVD is alarmingly high among diabetic individuals, particularly in North America and the Caribbean (46.0%), and Southeast Asia (42.5%). The predominant form of CVD among diabetic patients is coronary artery disease (CAD), accounting for 29.4% of cases. The pathophysiology of DM is complex, involving insulin resistance, β-cell dysfunction, and associated cardiovascular complications including diabetic cardiomyopathy (DCM) and cardiovascular autonomic neuropathy (CAN). These conditions exacerbate CVD risks underscoring the importance of managing key risk factors including hypertension, dyslipidemia, obesity, and genetic predisposition. Understanding the genetic networks and molecular processes that link diabetes and cardiovascular disease can lead to new diagnostics and therapeutic interventions. Imeglimin, a novel mitochondrial bioenergetic enhancer, represents a promising medication for diabetes with the potential to address both insulin resistance and secretion difficulties. Effective diabetes management through oral hypoglycemic agents (OHAs) can protect the cardiovascular system. Additionally, certain antihypertensive medications can significantly reduce the risk of diabetes-related CVD. Additionally, lifestyle changes, including diet and exercise are vital in managing diabesity and reducing CVD risks. These interventions, along with emerging therapeutic agents and ongoing clinical trials, offer hope for improved patient outcomes and long-term DM remission. This study highlights the urgent need for management strategies to address the overlapping epidemics of DM and CVD. By elucidating the underlying mechanisms and risk factors, this study aims to guide future perspectives and enhance understanding of the pathogenesis of CVD complications in patients with DM, thereby guiding more effective treatment strategies.
Keywords: cardiovascular and obesity; cardiovascular drugs; diabetes mellitus; hyperglycemia; hypertension; insulin resistance.
Copyright: © 2024 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- WHO. Global Health Estimates 2023. [(Accessed: 29 March 2024)]. Available at: https://www.who.int/data/global-health-estimates .
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
