

Long-term Follow-up Optical Coherence Tomography Assessment of Primary Percutaneous Coronary Intervention for Unprotected Left Main
- PMID: 39742225
- PMCID: PMC11683725
- DOI: 10.31083/j.rcm2512445
Long-term Follow-up Optical Coherence Tomography Assessment of Primary Percutaneous Coronary Intervention for Unprotected Left Main
Abstract
Background: Elective unprotected left main (ULM) percutaneous coronary intervention (PCI) has long-term mortality rates comparable to surgical revascularization, thanks to advances in drug-eluting stent (DES) design, improved PCI techniques, and frequent use of intravascular imaging. However, urgent PCI of ULM culprit lesions remains associated with high in-hospital mortality and unfavourable long-term outcomes, including DES restenosis and stent thrombosis (ST). This analysis aimed to examine the long-term outcomes and healing of DES implanted in ULM during primary PCI using high-resolution optical coherence tomography (OCT) imaging.
Methods: A total of 15 consecutive patients undergoing long-term OCT follow-up of ULM primary PCI from a high-volume center were included in this analysis. During the index primary PCI all subjects underwent angio-guided DES implantation, and follow-up was uneventful in all but one subject who had a non-target PCI lesion. The primary endpoint was the percentage of covered, uncovered, and malappossed stent struts at long-term follow-up. Secondary endpoints included quantitative and qualitative OCT measurements. For the left main bifurcation, a separate analysis was performed for three different segments: left main (LM), polygon of confluence (POC) and distal main branch (dMB), in all cases.
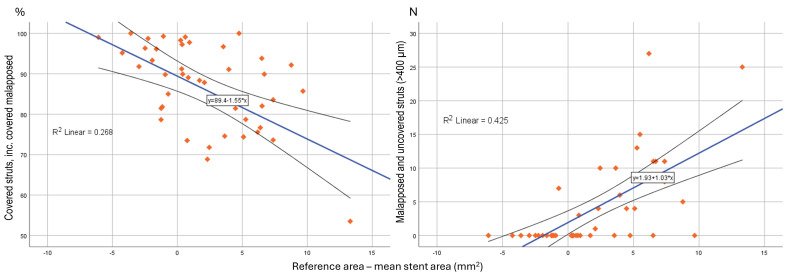
Results: The average follow-up interval until OCT was 1580 ± 1260 days. Despite aorto-ostial stent protrusions in 40% of patients, optimal image quality was achieved in 93.3% of cases. There were higher rates of malapposed (11.4 ± 16.6 vs. 13.1 ± 8.3 vs. 0.3 ± 0.5%; p < 0.001) and lower rates of covered struts (81.7 ± 16.8 vs. 83.7 ± 9.2 vs. 92.4 ± 6.8%; p = 0.041) observed for the LM and POC segment compared to the dMB. Significantly malapposed stent struts (>400 μm) were less likely to be covered at follow-up, than struts with a measured strut to vessel wall distance of <400 μm (15.4 ± 21.6 vs. 24.8 ± 23.9%; p = 0.011). Neoatherosclerosis was observed in 5 (33.3%) and restenotic neointimal hyperplasia (NIH) in 2 (13.3%) patients, requiring PCI in 33.3% of patients.
Conclusions: Long-term OCT examination of DES implanted during primary PCI for culprit ULM lesions demonstrated high rates of incomplete strut coverage, late malapposition, and high subclinical DES failure rates. These negative OCT results highlight the need for image optimization strategies during primary PCI to improve DES-related long-term outcomes.
Keywords: OCT; long-term follow-up; primary PCI; stent malapposition; strut endothelization; unprotected left main.
Copyright: © 2024 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
-
- Byrne RA, Fremes S, Capodanno D, Czerny M, Doenst T, Emberson JR, et al. 2022 Joint ESC/EACTS review of the 2018 guideline recommendations on the revascularization of left main coronary artery disease in patients at low surgical risk and anatomy suitable for PCI or CABG. European Journal of Cardio-Thoracic Surgery . 2023;64:ezad286. - PubMed
-
- Puricel S, Adorjan P, Oberhänsli M, Stauffer JC, Moschovitis A, Vogel R, et al. Clinical outcomes after PCI for acute coronary syndrome in unprotected left main coronary artery disease: insights from the Swiss Acute Left Main Coronary Vessel Percutaneous Management (SALVage) study. EuroIntervention: Journal of EuroPCR in Collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology . 2011;7:697–704. - PubMed
-
- Yeoh J, Andrianopoulos N, Reid CM, Yudi MB, Hamilton G, Freeman M, et al. Long-term outcomes following percutaneous coronary intervention to an unprotected left main coronary artery in cardiogenic shock. International Journal of Cardiology . 2020;308:20–25. - PubMed
-
- Homorodean C, Iancu AC, Leucuţa D, Bãlãnescu Ş, Dregoesc IM, Spînu M, et al. New Predictors of Early and Late Outcomes after Primary Percutaneous Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction and Unprotected Left Main Coronary Artery Culprit Lesion. Journal of Interventional Cardiology . 2019;2019:8238972. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
