

Global consensus on optimal exercise recommendations for enhancing healthy longevity in older adults (ICFSR)
- PMID: 39743381
- PMCID: PMC11812118
- DOI: 10.1016/j.jnha.2024.100401
Global consensus on optimal exercise recommendations for enhancing healthy longevity in older adults (ICFSR)
Abstract
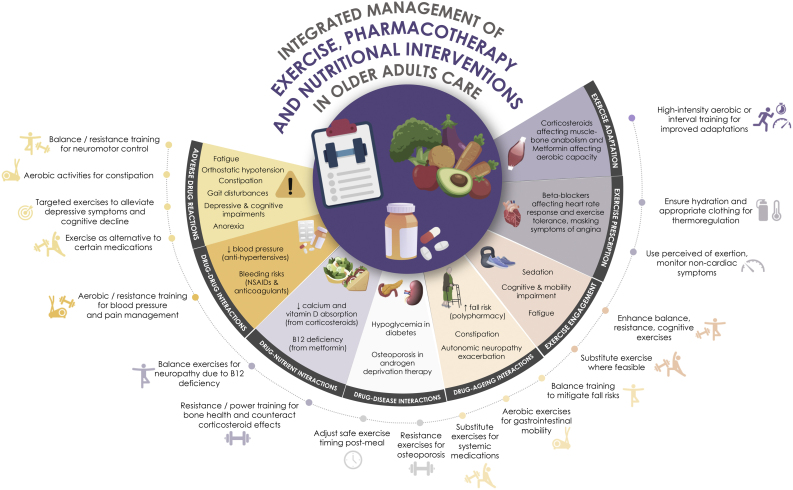
Aging, a universal and inevitable process, is characterized by a progressive accumulation of physiological alterations and functional decline over time, leading to increased vulnerability to diseases and ultimately mortality as age advances. Lifestyle factors, notably physical activity (PA) and exercise, significantly modulate aging phenotypes. Physical activity and exercise can prevent or ameliorate lifestyle-related diseases, extend health span, enhance physical function, and reduce the burden of non-communicable chronic diseases including cardiometabolic disease, cancer, musculoskeletal and neurological conditions, and chronic respiratory diseases as well as premature mortality. Physical activity influences the cellular and molecular drivers of biological aging, slowing aging rates-a foundational aspect of geroscience. Thus, PA serves both as preventive medicine and therapeutic agent in pathological states. Sub-optimal PA levels correlate with increased disease prevalence in aging populations. Structured exercise prescriptions should therefore be customized and monitored like any other medical treatment, considering the dose-response relationships and specific adaptations necessary for intended outcomes. Current guidelines recommend a multifaceted exercise regimen that includes aerobic, resistance, balance, and flexibility training through structured and incidental (integrated lifestyle) activities. Tailored exercise programs have proven effective in helping older adults maintain their functional capacities, extending their health span, and enhancing their quality of life. Particularly important are anabolic exercises, such as Progressive resistance training (PRT), which are indispensable for maintaining or improving functional capacity in older adults, particularly those with frailty, sarcopenia or osteoporosis, or those hospitalized or in residential aged care. Multicomponent exercise interventions that include cognitive tasks significantly enhance the hallmarks of frailty (low body mass, strength, mobility, PA level, and energy) and cognitive function, thus preventing falls and optimizing functional capacity during aging. Importantly, PA/exercise displays dose-response characteristics and varies between individuals, necessitating personalized modalities tailored to specific medical conditions. Precision in exercise prescriptions remains a significant area of further research, given the global impact of aging and broad effects of PA. Economic analyses underscore the cost benefits of exercise programs, justifying broader integration into health care for older adults. However, despite these benefits, exercise is far from fully integrated into medical practice for older people. Many healthcare professionals, including geriatricians, need more training to incorporate exercise directly into patient care, whether in settings including hospitals, outpatient clinics, or residential care. Education about the use of exercise as isolated or adjunctive treatment for geriatric syndromes and chronic diseases would do much to ease the problems of polypharmacy and widespread prescription of potentially inappropriate medications. This intersection of prescriptive practices and PA/exercise offers a promising approach to enhance the well-being of older adults. An integrated strategy that combines exercise prescriptions with pharmacotherapy would optimize the vitality and functional independence of older people whilst minimizing adverse drug reactions. This consensus provides the rationale for the integration of PA into health promotion, disease prevention, and management strategies for older adults. Guidelines are included for specific modalities and dosages of exercise with proven efficacy in randomized controlled trials. Descriptions of the beneficial physiological changes, attenuation of aging phenotypes, and role of exercise in chronic disease and disability management in older adults are provided. The use of exercise in cardiometabolic disease, cancer, musculoskeletal conditions, frailty, sarcopenia, and neuropsychological health is emphasized. Recommendations to bridge existing knowledge and implementation gaps and fully integrate PA into the mainstream of geriatric care are provided. Particular attention is paid to the need for personalized medicine as it applies to exercise and geroscience, given the inter-individual variability in adaptation to exercise demonstrated in older adult cohorts. Overall, this consensus provides a foundation for applying and extending the current knowledge base of exercise as medicine for an aging population to optimize health span and quality of life.
Copyright © 2024 The Author(s). Published by Elsevier Masson SAS.. All rights reserved.
Figures







References
-
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2019 (ST/ESA/SER.A/444). 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
