

Phenotyping atherosclerotic plaque and perivascular adipose tissue: signalling pathways and clinical biomarkers in atherosclerosis
- PMID: 39743563
- PMCID: PMC12092191
- DOI: 10.1038/s41569-024-01110-1
Phenotyping atherosclerotic plaque and perivascular adipose tissue: signalling pathways and clinical biomarkers in atherosclerosis
Abstract
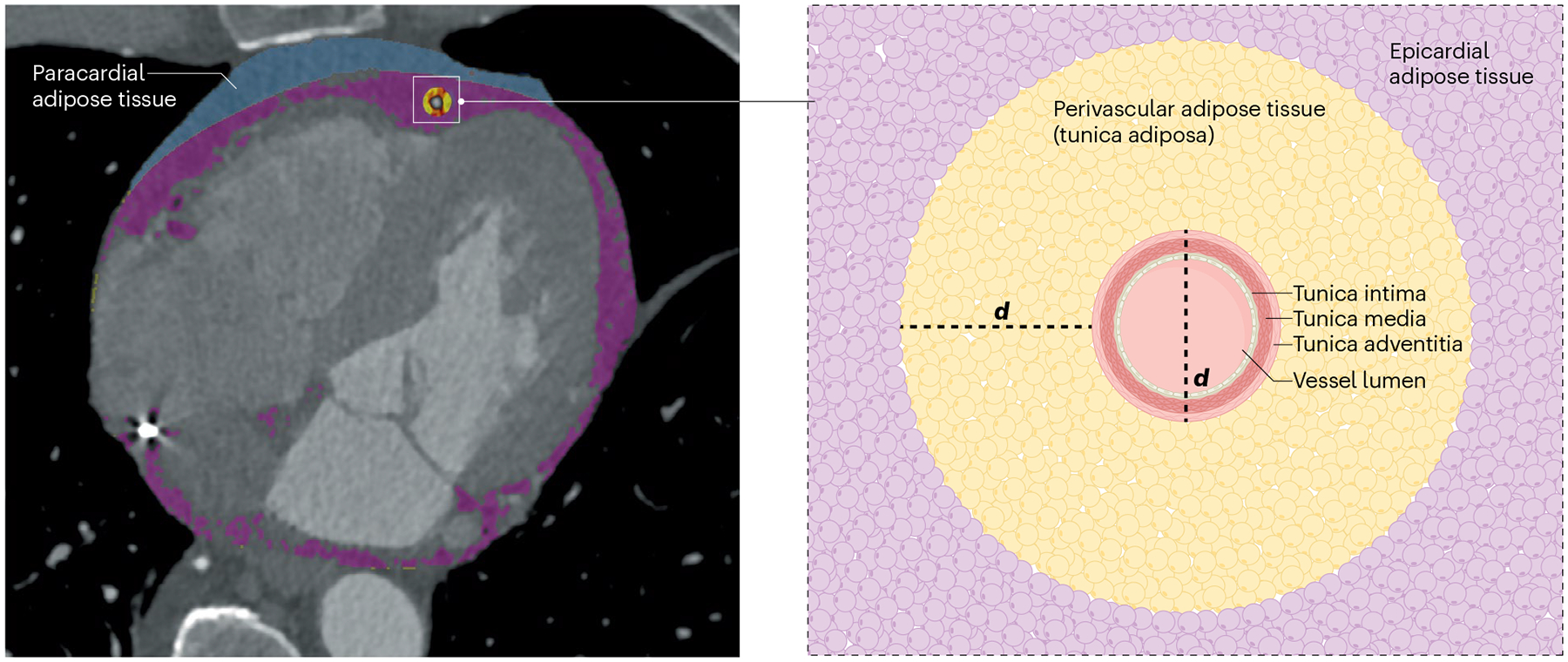
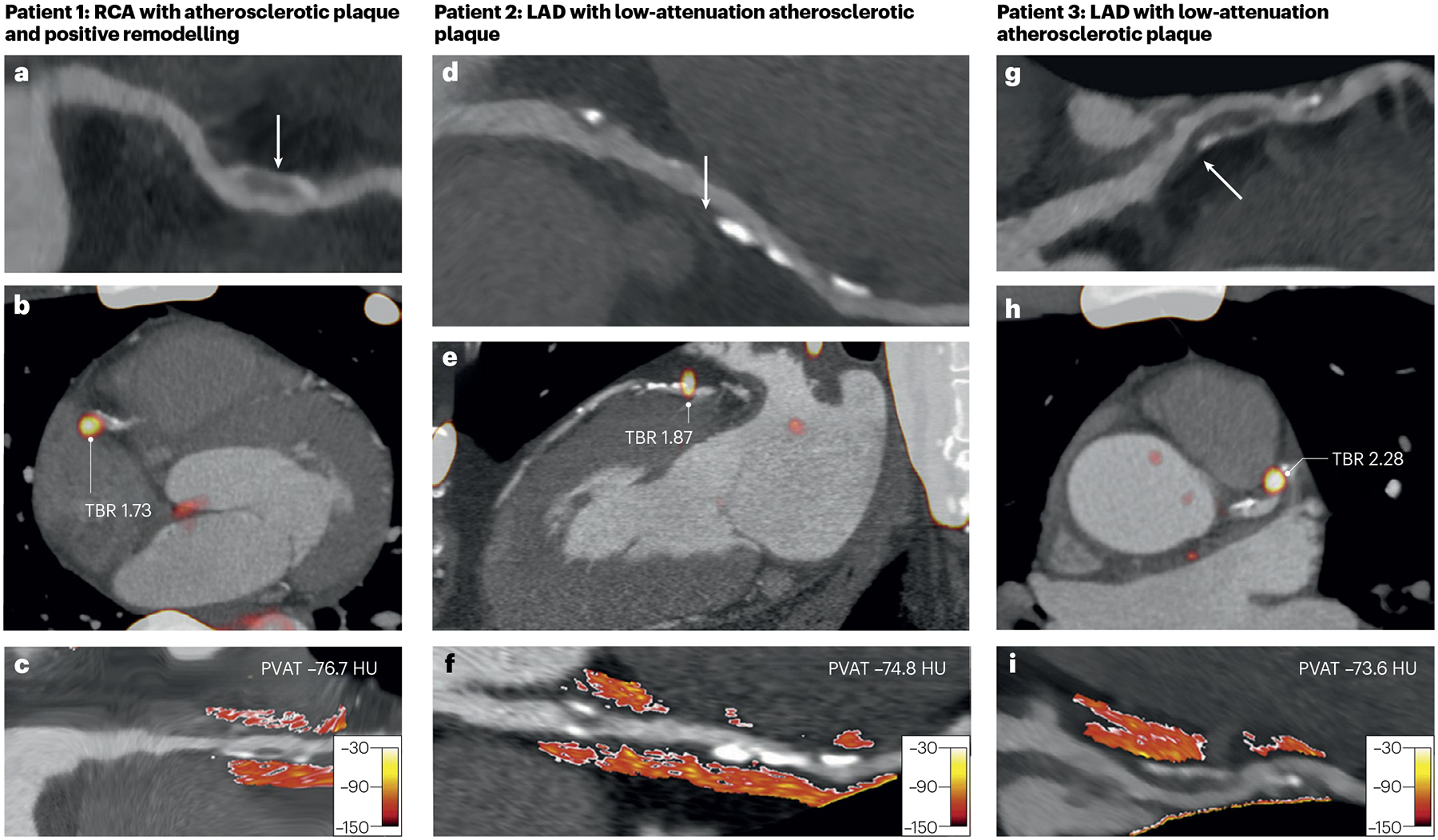
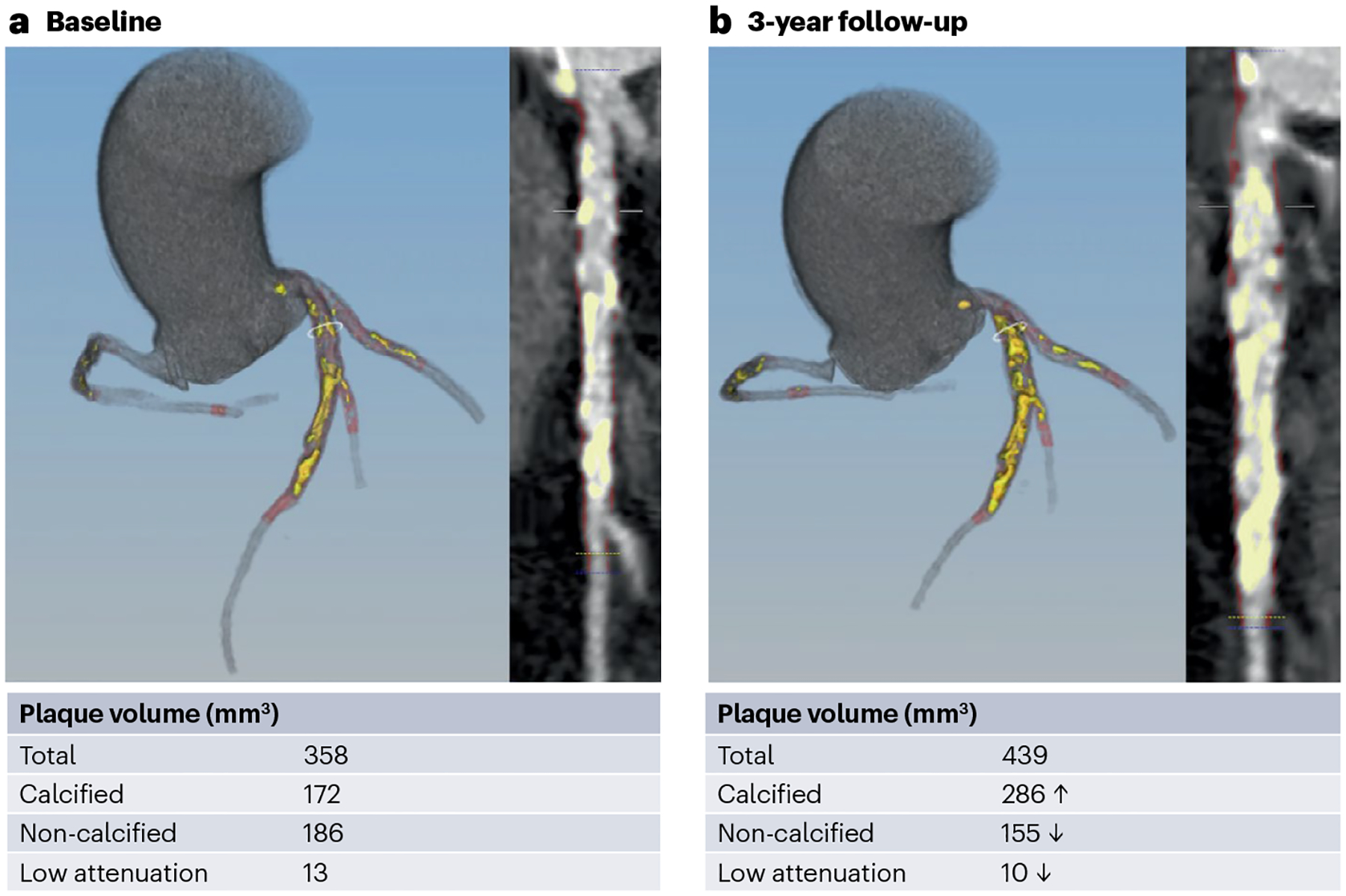
Computed tomography coronary angiography provides a non-invasive evaluation of coronary artery disease that includes phenotyping of atherosclerotic plaques and the surrounding perivascular adipose tissue (PVAT). Image analysis techniques have been developed to quantify atherosclerotic plaque burden and morphology as well as the associated PVAT attenuation, and emerging radiomic approaches can add further contextual information. PVAT attenuation might provide a novel measure of vascular health that could be indicative of the pathogenetic processes implicated in atherosclerosis such as inflammation, fibrosis or increased vascularity. Bidirectional signalling between the coronary artery and adjacent PVAT has been hypothesized to contribute to coronary artery disease progression and provide a potential novel measure of the risk of future cardiovascular events. However, despite the development of more advanced radiomic and artificial intelligence-based algorithms, studies involving large datasets suggest that the measurement of PVAT attenuation contributes only modest additional predictive discrimination to standard cardiovascular risk scores. In this Review, we explore the pathobiology of coronary atherosclerotic plaques and PVAT, describe their phenotyping with computed tomography coronary angiography, and discuss potential future applications in clinical risk prediction and patient management.
© 2025. Springer Nature Limited.
Conflict of interest statement
Competing interests: P.J.S., D.B. and D.D. may receive royalties from Cedars-Sinai Medical Center and have equity in APQ Health. The other authors declare no competing interests.
Figures


References
-
- Vaduganathan M, Mensah GA, Turco JV, Fuster V & Roth GA The global burden of cardiovascular diseases and risk. J. Am. Coll. Cardiol 80, 2361–2371 (2022). - PubMed
-
- Ibanez B et al. Progression of early subclinical atherosclerosis (PESA) study. J. Am. Coll. Cardiol 78, 156–179 (2021). - PubMed
-
- Libby P et al. Atherosclerosis. Nat. Rev. Dis. Prim 5, 56 (2019). - PubMed
-
- Falk E, Shah PK & Fuster V Coronary plaque disruption. Circulation 92, 657–671 (1995). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
