

Serum fatty acid profiles in systemic lupus erythematosus and patient reported outcomes: The Michigan Lupus Epidemiology & Surveillance (MILES) Program
- PMID: 39744623
- PMCID: PMC11688325
- DOI: 10.3389/fimmu.2024.1459297
Serum fatty acid profiles in systemic lupus erythematosus and patient reported outcomes: The Michigan Lupus Epidemiology & Surveillance (MILES) Program
Abstract
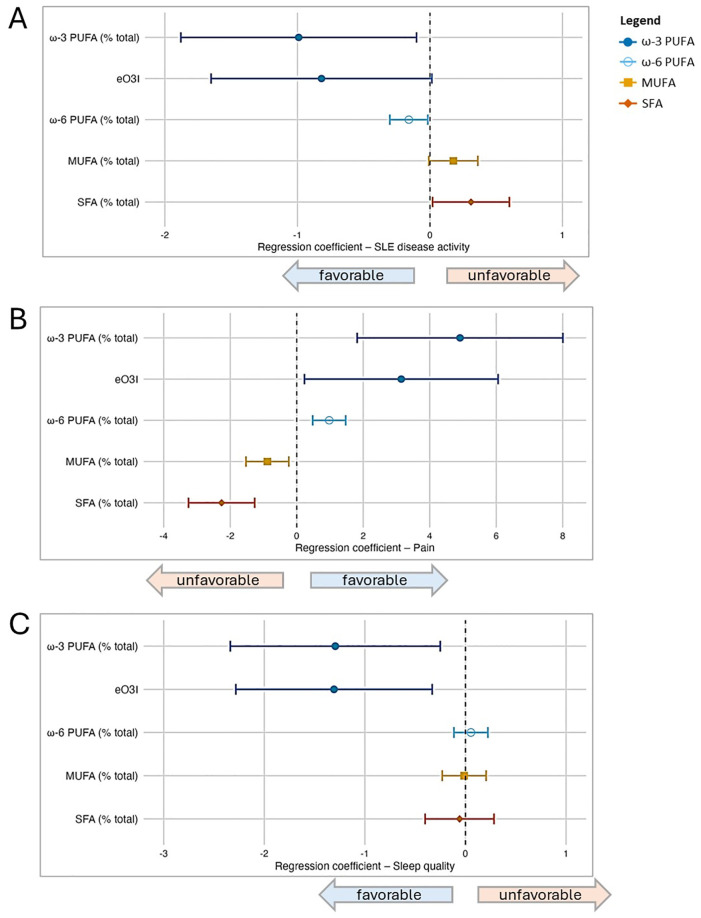
Introduction: Despite progress in systemic lupus erythematosus (SLE) treatment, challenges persist in medication adherence due to side effects and costs. Precision nutrition, particularly adjusting fatty acid intake, offers a cost-effective strategy for enhancing SLE management. Prior research, including our own, indicates that increased consumption of omega-3 polyunsaturated fatty acids (PUFAs) correlates with improved outcomes in SLE patients. Here we build upon these findings by investigating associations between serum fatty acids-grouped as PUFAs, monounsaturated fatty acids (MUFAs), and saturated fatty acids (SFAs)-and lupus activity, pain, and sleep disturbance.
Methods: Using data from 418 participants with SLE in the Michigan Lupus Epidemiology and Surveillance (MILES) Cohort, we examined associations between serum levels of 25 fatty acids determined by GC-MS and patient-reported outcomes. Disease activity, pain, and sleep quality were assessed using standardized questionnaires. Generalized additive models and partial residual plots were utilized to examine the linearity of fatty acid effects. Variable selection was performed using Least Absolute Shrinkage and Selection Operator (LASSO), followed by multiple linear regression adjusting for sociodemographic factors.
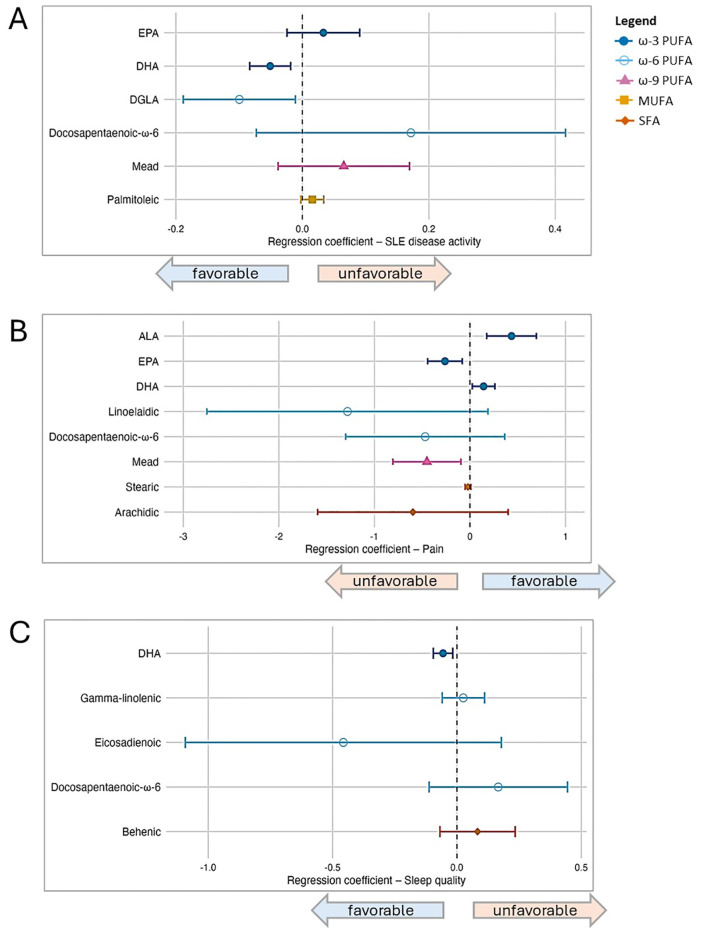
Results: Findings indicated favorable associations between ω-3 PUFAs-and, to a lesser extent, ω-6 PUFAs-and patient-reported outcomes, while MUFAs and SFAs showed unfavorable associations. Docosahexaenoic acid (DHA), an omega-3 PUFA, exhibited the most robust favorable associations across all outcomes. Additionally, the omega-3 α-linolenic acid (ALA) was linked to reduced pain, whereas eicosapentaenoic acid (EPA), another omega-3, was associated with worsened disease activity and pain. Among omega-6 PUFAs, dihomo-γ-linolenic acid (DGLA) was favorably associated with disease activity, while the omega-9 PUFA Mead acid was linked to increased pain.
Discussion: These findings underscore the prospect that increased tissue levels of long-chain omega-3 PUFAs, particularly DHA, are favorably associated with SLE outcomes. Although further research is needed to establish causal relationships, existing evidence supports the role of omega-3 PUFAs in managing cardiovascular and chronic kidney disease, common SLE comorbidities. Most study participants exhibited low omega-3 PUFA status, suggesting substantial potential for improvement through targeted dietary interventions and supplementation. This study supports a potential role for precision nutrition in comprehensive SLE management, considering the impact of PUFAs, SFAs and MUFAs.
Keywords: autoimmune; docosahexaenoic acid (DHA); monounsaturated fatty acid (MUFA); omega-3 fatty acid; pain; polyunsaturated fatty acid (PUFA); saturated fatty acid (SFA); sleep.
Copyright © 2024 Gilley, Fenton, Zick, Li, Wang, Marder, McCune, Jain, Herndon-Fenton, Hassett, Barbour, Pestka and Somers.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
Similar articles
-
Polyunsaturated fatty acid supplementation for drug-resistant epilepsy.Cochrane Database Syst Rev. 2016 Aug 17;2016(8):CD011014. doi: 10.1002/14651858.CD011014.pub2. Cochrane Database Syst Rev. 2016. PMID: 27536971 Free PMC article.
-
Omega-3 fatty acid supplementation for depression in children and adolescents.Cochrane Database Syst Rev. 2024 Nov 20;11(11):CD014803. doi: 10.1002/14651858.CD014803.pub2. Cochrane Database Syst Rev. 2024. PMID: 39564892
-
Association between polyunsaturated fatty acids intake and serum neurofilament light chain concentrations in American adults: a cross-sectional study.Front Nutr. 2025 Jul 11;12:1608211. doi: 10.3389/fnut.2025.1608211. eCollection 2025. Front Nutr. 2025. PMID: 40717996 Free PMC article.
-
Omega-3 fatty acids for the treatment of dementia.Cochrane Database Syst Rev. 2016 Apr 11;4(4):CD009002. doi: 10.1002/14651858.CD009002.pub3. Cochrane Database Syst Rev. 2016. PMID: 27063583 Free PMC article.
-
Omega-3 fatty acids for the primary and secondary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2018 Jul 18;7(7):CD003177. doi: 10.1002/14651858.CD003177.pub3. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2018 Nov 30;11:CD003177. doi: 10.1002/14651858.CD003177.pub4. PMID: 30019766 Free PMC article. Updated.
Cited by
-
Serum untargeted metabolomics alterations in systemic lupus erythematosus patients with elevated serum ferritin.Sci Rep. 2025 Jul 15;15(1):25481. doi: 10.1038/s41598-025-06170-y. Sci Rep. 2025. PMID: 40664755 Free PMC article.
References
-
- Sammaritano LR, Bermas BL, Chakravarty EE, Chambers C, Clowse MEB, Lockshin MD, et al. . 2020 American College of Rheumatology Guideline for the management of reproductive health in rheumatic and musculoskeletal diseases. Arthritis Rheumatol (Hoboken NJ). (2020) 72:529–56. doi: 10.1002/art.41191 - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous