

Structurally Oriented Classification of FOXA1 Alterations Identifies Prostate Cancers with Opposing Clinical Outcomes and Distinct Molecular and Immunologic Subtypes
- PMID: 39745364
- PMCID: PMC11873805
- DOI: 10.1158/1078-0432.CCR-24-3471
Structurally Oriented Classification of FOXA1 Alterations Identifies Prostate Cancers with Opposing Clinical Outcomes and Distinct Molecular and Immunologic Subtypes
Abstract
Purpose: Around 10% to 15% of prostate cancers harbor recurrent aberrations in the Forkhead Box A1 gene, FOXA1, whereby the alteration type and the effect on the forkhead (FKH) domain affect protein function. We developed a FOXA1 classification system to inform clinical management.
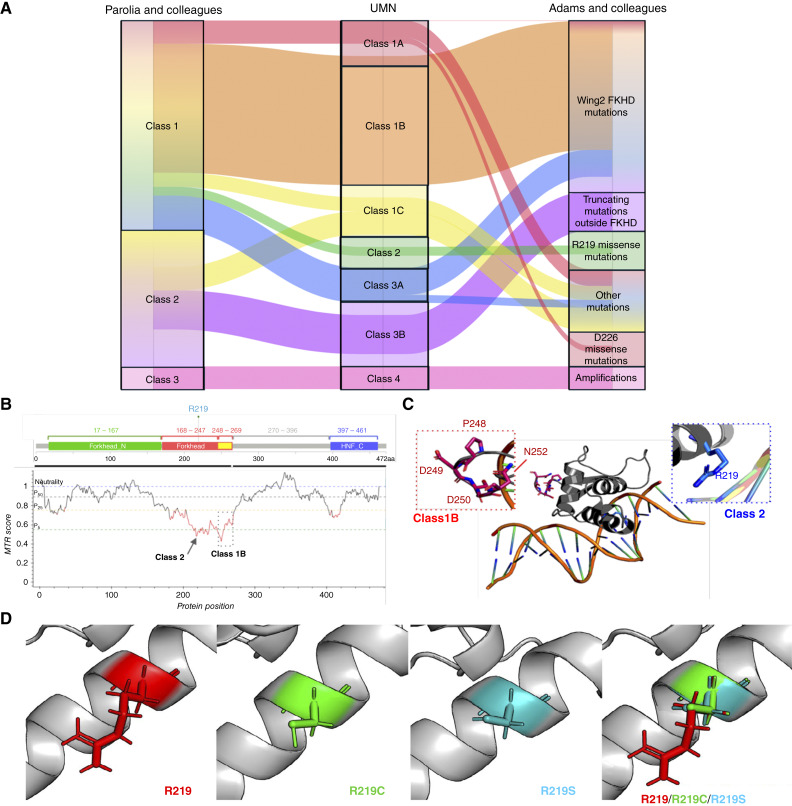
Experimental design: A total of 5,014 prostate cancer samples were examined using whole-exome and -transcriptome sequencing from the Caris Life Sciences database. We denoted class 1 FOXA1 alterations as missense and in-frame insertions/deletions with subclasses oriented with respect to the FKH domain. These were in the first part of the FKH domain [class 1A: amino acids (AA) 168-246], within the Wing2 region of FKH (class 1B: AA 247-269), or outside FKH (class 1C: AA 1-167, 270+). Two hotspot missense mutations at R219 were denoted class 2. Class 3 included predicted truncating mutations with subclasses partitioned based on the FKH domain (class 3A: AA 1-269 and class 3B: AA 270+). Class 4 represented FOXA1 amplifications. Real-world overall survival and therapy outcomes were determined from insurance claims.
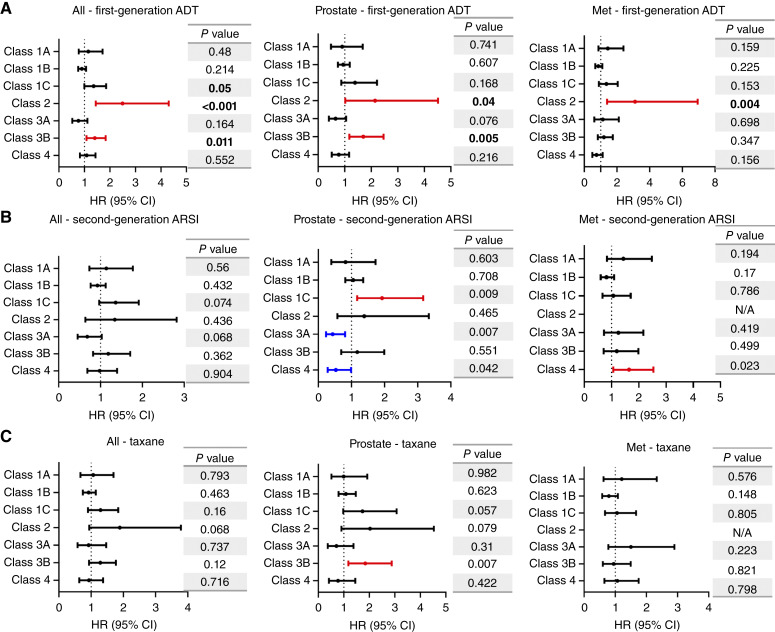
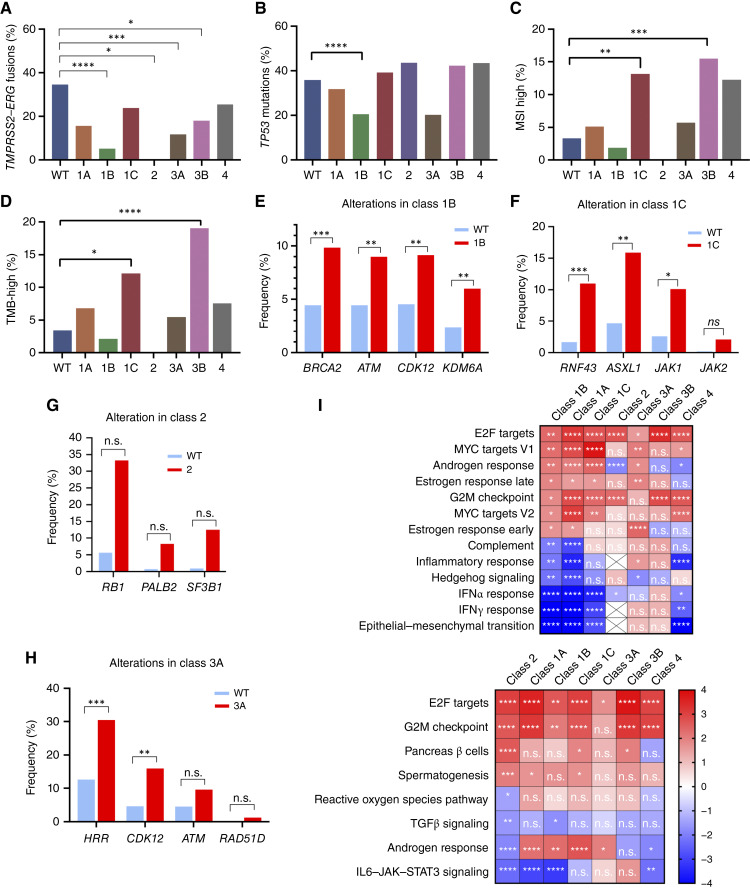
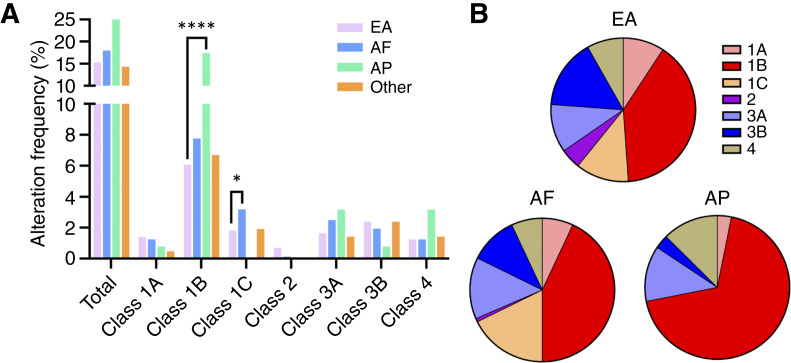
Results: FOXA1 alterations did not influence survival when considered in aggregate but had distinct prognostic effects when stratified by class. In primary prostate samples, class 1A alterations were associated with overall improved survival (HR, 0.57; P = 0.03); a similar trend was seen in metastatic biopsies with class 1B (HR, 0.84; P = 0.09). Conversely, in primary specimens, class 1C exhibited worse survival upon second-generation androgen receptor signaling inhibitor treatment (HR, 1.93; P < 0.001). Class 2 mutations (R219C/S) were enriched in neuroendocrine prostate cancers and were associated with overall poor survival (HR, 2.05; P < 0.001) and worse outcomes to first-line androgen-deprivation therapies (HR, 2.5; P < 0.001). Class 3A alterations indicated improved survival (HR, 0.70; P = 0.01), whereas class 3B alterations portended poor outcomes (HR, 1.50; P < 0.001). Amplifications (class 4) indicated poor outcomes in metastatic samples (HR, 1.48; P = 0.02). Molecularly, different FOXA1 alteration classes harbored distinct mutational and immunologic features as well as unique transcriptional programs. Finally, relative to European Americans, African Americans had increased class 1C alterations, whereas Asian/Pacific Islander patients had increased class 1B alterations.
Conclusions: FOXA1 alterations should not be interpreted in aggregate, as different classes are associated with divergent molecular features and clinical outcomes. Our revised classification schema facilitates clinical decision-making for patients with prostate cancer and uncovers important racial differences.
©2025 The Authors; Published by the American Association for Cancer Research.
Conflict of interest statement
S. Wu reports other support from Caris Life Sciences during the conduct of the study. J.J. Kwon reports grants from NCI/NIH during the conduct of the study, as well as personal fees from A2A Pharmaceuticals outside the submitted work and employment with AbbVie. D. Moline reports personal fees from Tempus outside the submitted work. M.G. Evans reports personal fees from Caris Life Sciences outside the submitted work. A. Elliott reports personal fees from Caris Life Sciences during the conduct of the study. R.R. McKay reports serving as a consultant/advisor for Ambrx, Arcus, AstraZeneca, Aveo, Bayer, Blue Earth Diagnostics, Bristol Myers Squibb, Calithera, Caris, Daiichi Sankyo, Dendreon, Exelixis, Johnson & Johnson, Eli Lilly, Merck, Myovant, Neomorph, Novartis, Pfizer, Sanofi, Seagen, Sorrento Therapeutics, Telix, and Tempus and receives institutional research funding from Artera AI, AstraZeneca, Bayer, Bristol Myers Squibb, Exelixis, Oncternal, and Tempus. C. Nabhan reports other support from Caris Life Sciences during the conduct of the study. N. Reizine reports personal fees from Tempus, AstraZeneca, and Janssen outside the submitted work. J.J. Orme reports grants from the Prostate Cancer Foundation, Department of Defense, and NCI during the conduct of the study. S.M. Dehm reports personal fees from Bristol Myers Squibb/Celgene and Oncternal Therapeutics outside the submitted work. E.S. Antonarakis reports grants and personal fees from Janssen, Sanofi, Bayer, Bristol Myers Squibb, Curium, Merck, Pfizer, AstraZeneca, Clovis, and Constellation; personal fees from Astellas, Amgen, Blue Earth, Exact Sciences, Invitae, Eli Lilly, and Foundation Medicine; and grants from Novartis, Celgene, and Orion outside the submitted work, as well as a patent for an AR-V7 biomarker technology issued and licensed to Qiagen. No disclosures were reported by the other authors.
Figures


Similar articles
-
Distinct structural classes of activating FOXA1 alterations in advanced prostate cancer.Nature. 2019 Jul;571(7765):413-418. doi: 10.1038/s41586-019-1347-4. Epub 2019 Jun 26. Nature. 2019. PMID: 31243372 Free PMC article.
-
Pan-cancer genomic analysis reveals FOXA1 amplification is associated with adverse outcomes in non-small cell lung, prostate, and breast cancers.J Natl Cancer Inst. 2025 Jan 1;117(1):188-197. doi: 10.1093/jnci/djae224. J Natl Cancer Inst. 2025. PMID: 39254651
-
FOXA1 mutations alter pioneering activity, differentiation and prostate cancer phenotypes.Nature. 2019 Jul;571(7765):408-412. doi: 10.1038/s41586-019-1318-9. Epub 2019 Jun 26. Nature. 2019. PMID: 31243370 Free PMC article.
-
Pioneer of prostate cancer: past, present and the future of FOXA1.Protein Cell. 2021 Jan;12(1):29-38. doi: 10.1007/s13238-020-00786-8. Epub 2020 Sep 18. Protein Cell. 2021. PMID: 32946061 Free PMC article. Review.
-
FOXA1 in prostate cancer.Asian J Androl. 2023 May-Jun;25(3):287-295. doi: 10.4103/aja202259. Asian J Androl. 2023. PMID: 36018068 Free PMC article. Review.
Cited by
-
SOX2 utilizes FOXA1 as a heteromeric transcriptional partner to drive proliferation in therapy-resistant prostate cancer.bioRxiv [Preprint]. 2025 Jul 19:2025.07.18.664790. doi: 10.1101/2025.07.18.664790. bioRxiv. 2025. PMID: 40791379 Free PMC article. Preprint.
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–49. - PubMed
-
- Jozwik KM, Carroll JS. Pioneer factors in hormone-dependent cancers. Nat Rev Cancer 2012;12:381–5. - PubMed
MeSH terms
Substances
Grants and funding
- R37 CA288972/CA/NCI NIH HHS/United States
- P30 CA077598/CA/NCI NIH HHS/United States
- CRTI TWG/Masonic Cancer Center, University of Minnesota (MCC)
- 1R37CA288972-01/Division of Cancer Prevention, National Cancer Institute (DCP, NCI)
- Young Investigator Award/Prostate Cancer Foundation (PCF)
- K99 CA270290/CA/NCI NIH HHS/United States
- W81XWH-21-1-0358/U.S. Department of Defense (DOD)
- 1K99CA270290/Division of Cancer Prevention, National Cancer Institute (DCP, NCI)
- W81XWH-22-2-0025/U.S. Department of Defense (DOD)
- Innovation in Cancer Informatics/Damon Runyon Cancer Research Foundation (DRCRF)
LinkOut - more resources
Full Text Sources
Medical
