

Artificial Intelligence-Enhanced Electrocardiography for Prediction of Incident Hypertension
- PMID: 39745684
- PMCID: PMC11904724
- DOI: 10.1001/jamacardio.2024.4796
Artificial Intelligence-Enhanced Electrocardiography for Prediction of Incident Hypertension
Abstract
Importance: Hypertension underpins significant global morbidity and mortality. Early lifestyle intervention and treatment are effective in reducing adverse outcomes. Artificial intelligence-enhanced electrocardiography (AI-ECG) has been shown to identify a broad spectrum of subclinical disease and may be useful for predicting incident hypertension.
Objective: To develop an AI-ECG risk estimator (AIRE) to predict incident hypertension (AIRE-HTN) and stratify risk for hypertension-associated adverse outcomes.
Design, setting, and participants: This was a development and external validation prognostic cohort study conducted at Beth Israel Deaconess Medical Center (BIDMC) in Boston, Massachusetts, a secondary care setting. External validation was conducted in the UK Biobank (UKB), a UK-based volunteer cohort. AIRE-HTN was trained and tested to predict incident hypertension using routinely collected ECGs from patients at BIDMC between 2014 and 2023. The algorithm was then evaluated to risk stratify patients for hypertension- associated adverse outcomes and externally validated on UKB data between 2014 and 2022 for both incident hypertension and risk stratification.
Main outcomes and measures: AIRE-HTN, which uses a residual convolutional neural network architecture with a discrete-time survival loss function, was trained to predict incident hypertension.
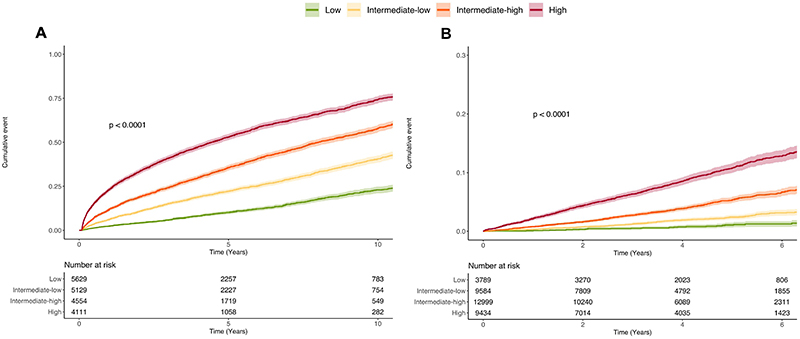
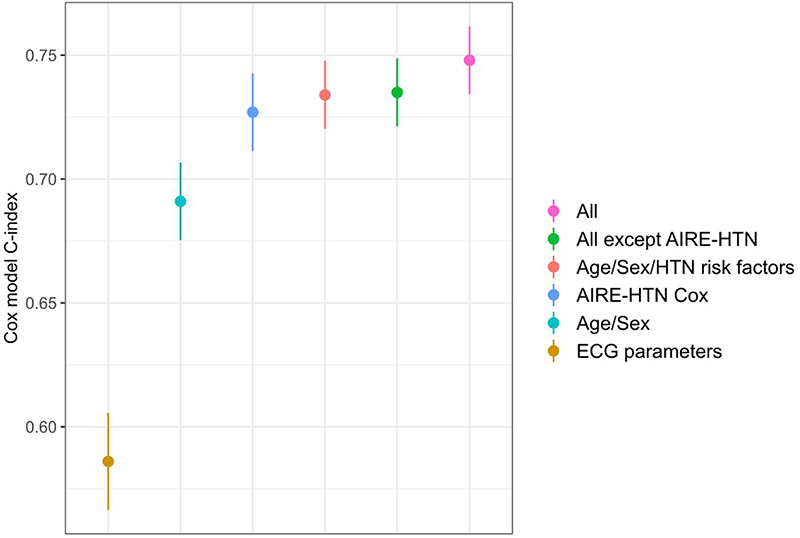
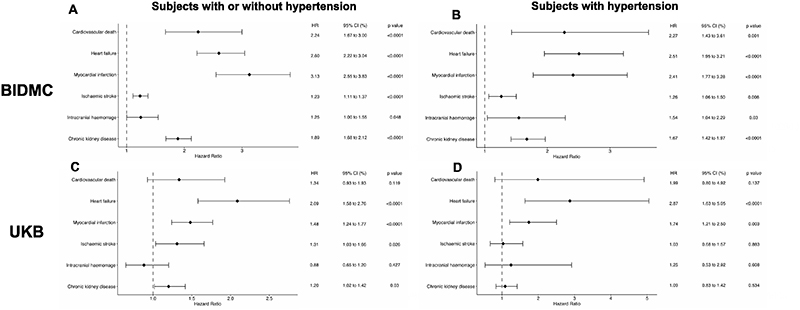
Results: AIRE-HTN was trained on 1 163 401 ECGs from 189 539 patients (mean [SD] age, 57.7 [18.7] years; 98 747 female [52.1%]) at BIDMC. A total of 19 423 BIDMC patients composed the test set and were evaluated for incident hypertension. From the UKB, AIRE-HTN was tested on 65 610 ECGs from same number of participants (mean [SD] age, 65.4 [7.9] years; 33 785 female [51.5%]). A total of 35 806 UKB patients were evaluated for incident hypertension. AIRE-HTN predicted incident hypertension (BIDMC: n = 6446 [33%] events; C index, 0.70; 95% CI, 0.69-0.71; UKB: n = 1532 [4%] events; C index, 0.70; 95% CI, 0.69-0.71). Performance was maintained in individuals without left ventricular hypertrophy and those with normal ECGs (C indices, 0.67-0.72). AIRE-HTN was significantly additive to existing clinical risk factors in predicting incident hypertension (continuous net reclassification index, BIDMC: 0.44; 95% CI, 0.33-0.53; UKB: 0.32; 95% CI, 0.23-0.37). In adjusted Cox models, AIRE-HTN score was an independent predictor of cardiovascular death (hazard ratio [HR] per standard deviation, 2.24; 95% CI, 1.67-3.00) and stratified risk for heart failure (HR, 2.60; 95% CI, 2.22-3.04), myocardial infarction (HR, 3.13; 95% CI, 2.55-3.83), ischemic stroke (HR, 1.23; 95% CI, 1.11-1.37), and chronic kidney disease (HR, 1.89; 95% CI, 1.68-2.12), beyond traditional risk factors.
Conclusions and relevance: Results suggest that AIRE-HTN, an AI-ECG model, can predict incident hypertension and identify patients at risk of hypertension-related adverse events, beyond conventional clinical risk factors.
Figures
References
-
- National Center for Health Statistics. [Accessed February 2, 2023];Multiple Cause of Death 2018−2021 on CDC WONDER Database.
-
- Global report on hypertension: the race against a silent killer. World Health Organization; Geneva: 2023. Licence: CC BY-NC-SA 3.0 IGO.
-
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. European Heart Journal. 2018 Aug 25;39(33):3021–104. - PubMed
-
- Verdecchia P, Schillaci G, Borgioni C, Ciucci A, Battistelli M, Bartoccini C, Santucci A, Santucci C, Reboldi G, Porcellati C. Left ventricular geometry as an independent predictor for extracardiac target organ damage in essential hypertension. Hypertension. 1998;31(5):1175–82. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
