

Predicting pediatric patient rehabilitation outcomes after spinal deformity surgery with artificial intelligence
- PMID: 39747461
- PMCID: PMC11697361
- DOI: 10.1038/s43856-024-00726-1
Predicting pediatric patient rehabilitation outcomes after spinal deformity surgery with artificial intelligence
Abstract
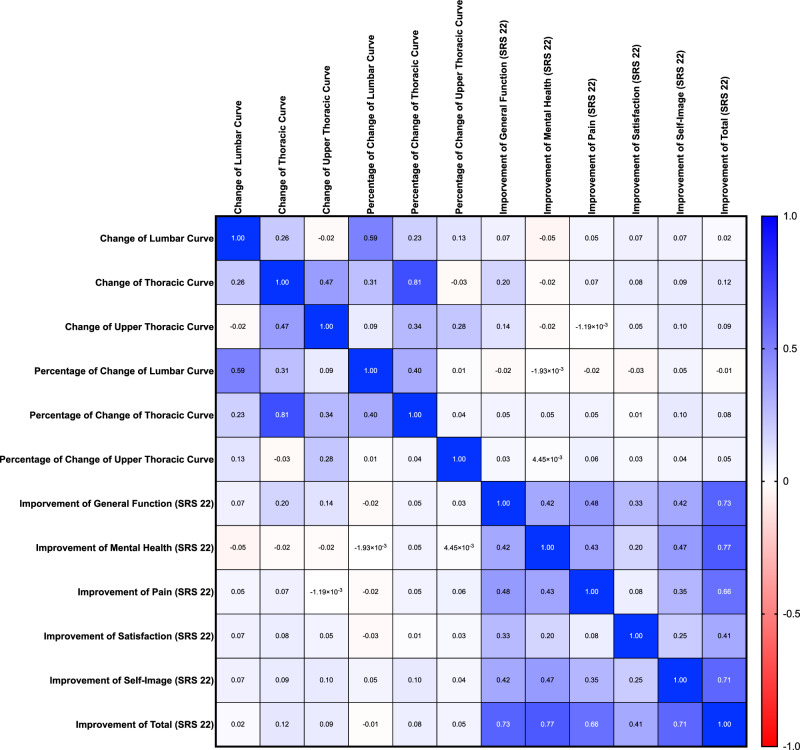
Background: Adolescent idiopathic scoliosis (AIS) is the most common type of scoliosis, affecting 1-4% of adolescents. The Scoliosis Research Society-22R (SRS-22R), a health-related quality-of-life instrument for AIS, has allowed orthopedists to measure subjective patient outcomes before and after corrective surgery beyond objective radiographic measurements. However, research has revealed that there is no significant correlation between the correction rate in major radiographic parameters and improvements in patient-reported outcomes (PROs), making it difficult to incorporate PROs into personalized surgical planning.
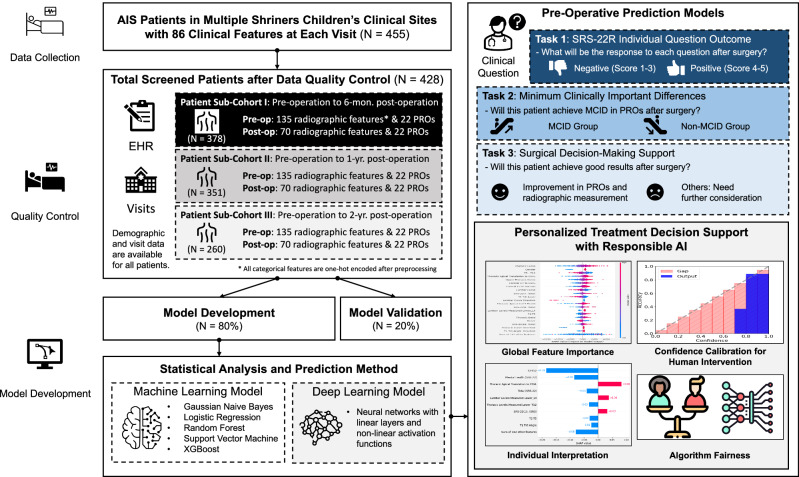
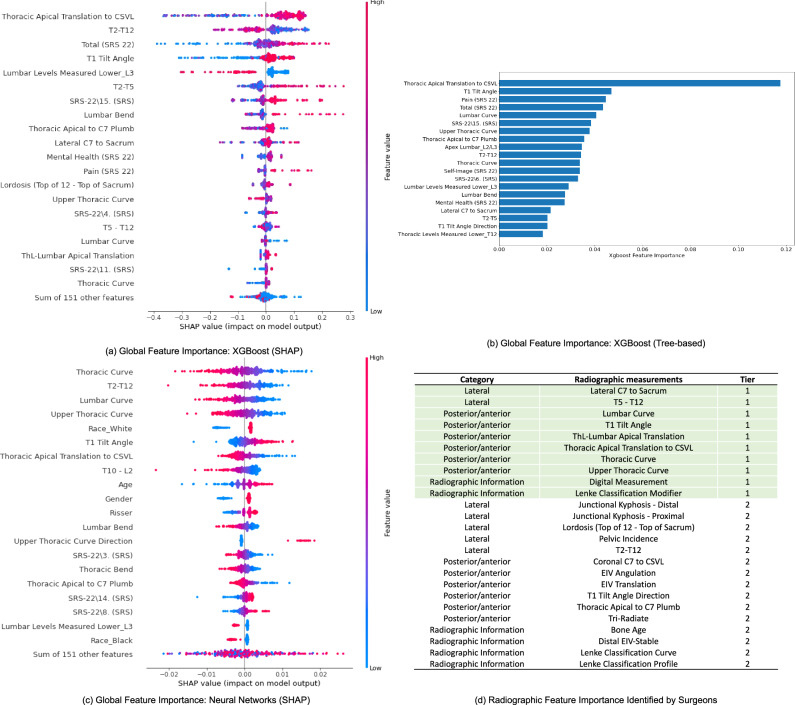
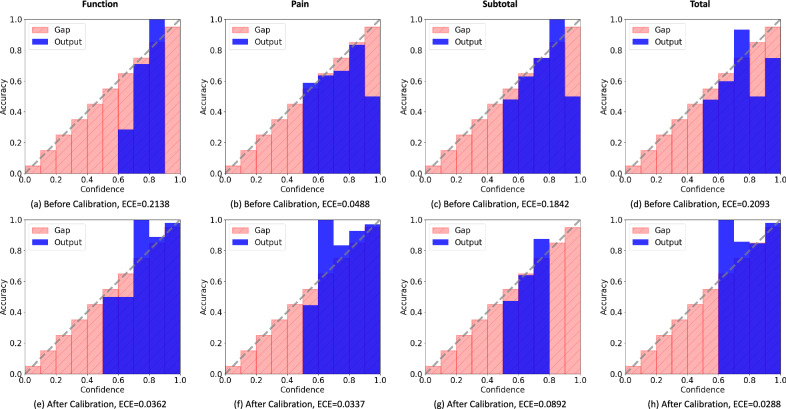
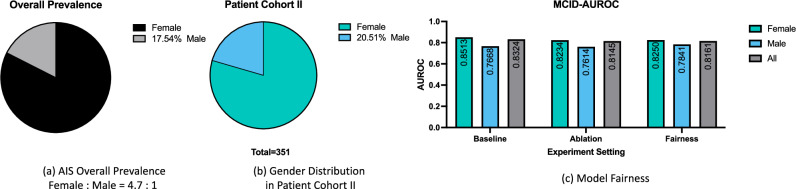
Methods: The objective of this study is to develop an artificial intelligence (AI)-enabled surgical planning and counseling support system for post-operative patient rehabilitation outcomes prediction in order to facilitate personalized AIS patient care. A unique multi-site cohort of 455 pediatric patients undergoing spinal fusion surgery at two Shriners Children's hospitals from 2010 is investigated in our analysis. In total, 171 pre-operative clinical features are used to train six machine-learning models for post-operative outcomes prediction. We further employ explainability analysis to quantify the contribution of pre-operative radiographic and questionnaire parameters in predicting patient surgical outcomes. Moreover, we enable responsible AI by calibrating model confidence for human intervention and mitigating health disparities for algorithm fairness.
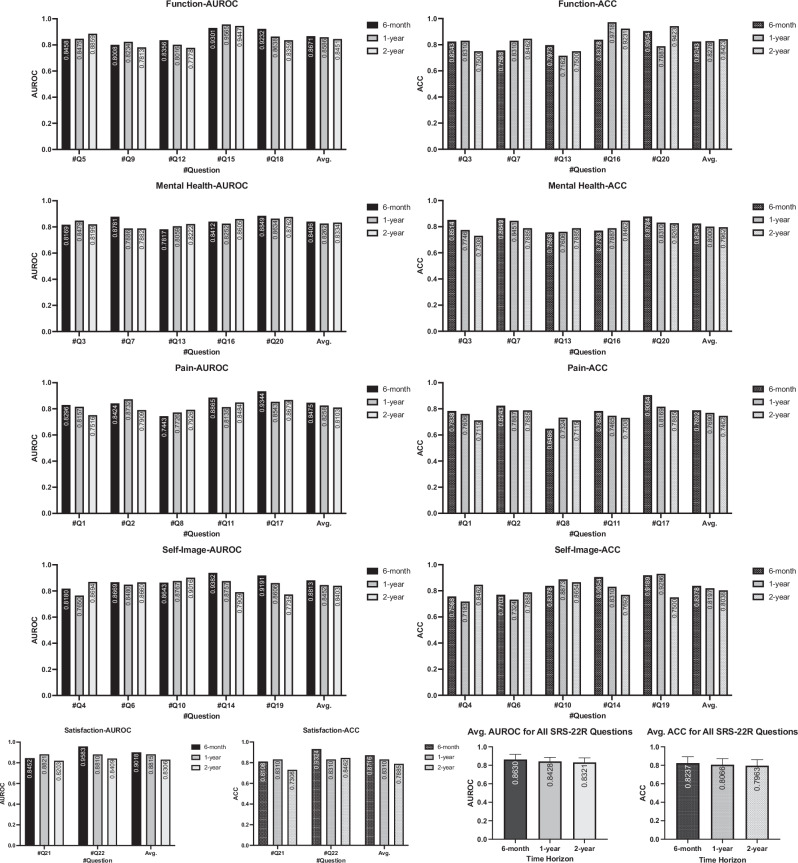
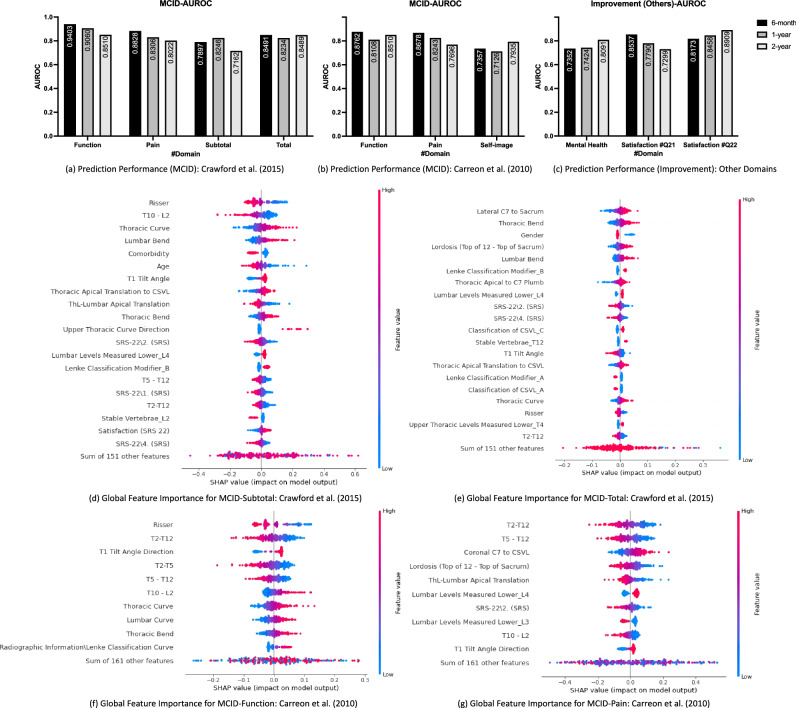
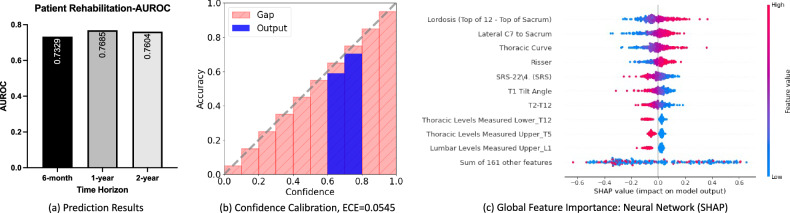
Results: The best prediction model achieves an area under receiver operating curve (AUROC) performance of 0.86, 0.85, and 0.83 for individual SRS-22R question response prediction over three-time horizons from pre-operation to 6-month, 1-year, and 2-year post-operation, respectively. Additionally, we demonstrate the efficacy of our proposed prediction method to predict other patient rehabilitation outcomes based on minimal clinically important differences (MCID) and correction rates across all three-time horizons.
Conclusions: Based on the relationship analysis, we suggest additional attention to sagittal parameters (e.g., lordosis, sagittal vertical axis) and patient self-image beyond major Cobb angles to improve surgical decision-making for AIS patients. In the age of personalized medicine, the proposed responsible AI-enabled clinical decision-support system may facilitate pre-operative counseling and shared decision-making within real-world clinical settings.
Plain language summary
The goal of this study is to develop a planning and counseling support system for predicting how well patients recover after surgeries. This should allow for more personalized care for scoliosis (spinal curvature) patients. We collected data from 455 pediatric patients who underwent spinal fusion surgery at different locations and used this data to train computer learning methods to predict outcomes after surgery. We show that our proposed computer method can predict the outcome of patient rehabilitation well for short-term (6-month and 1-year) and long-term (2-year) results. We applied additional tests to our method to calculate how well it works and measure fairness to provide a straight-forward, trustworthy, and fair method for real-world clinical use.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures
References
-
- Cheng, J. C. et al. Adolescent idiopathic scoliosis. Nat. Rev. Dis. Prim.1, 1–21 (2015). - PubMed
-
- White, A. Physical properties and functional biomechanics of the spine. Clin. Biomech. Spine22 278–283 (1990).
LinkOut - more resources
Full Text Sources
Miscellaneous
