

International multicenter validation of AI-driven ultrasound detection of ovarian cancer
- PMID: 39747679
- PMCID: PMC11750711
- DOI: 10.1038/s41591-024-03329-4
International multicenter validation of AI-driven ultrasound detection of ovarian cancer
Abstract
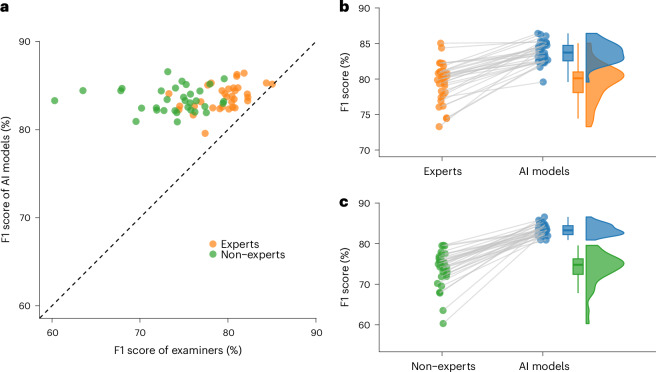
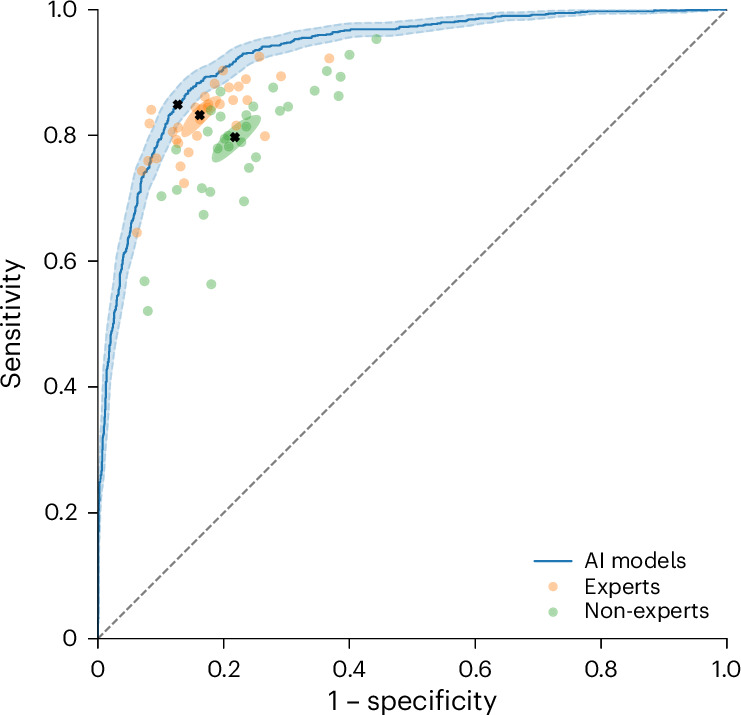
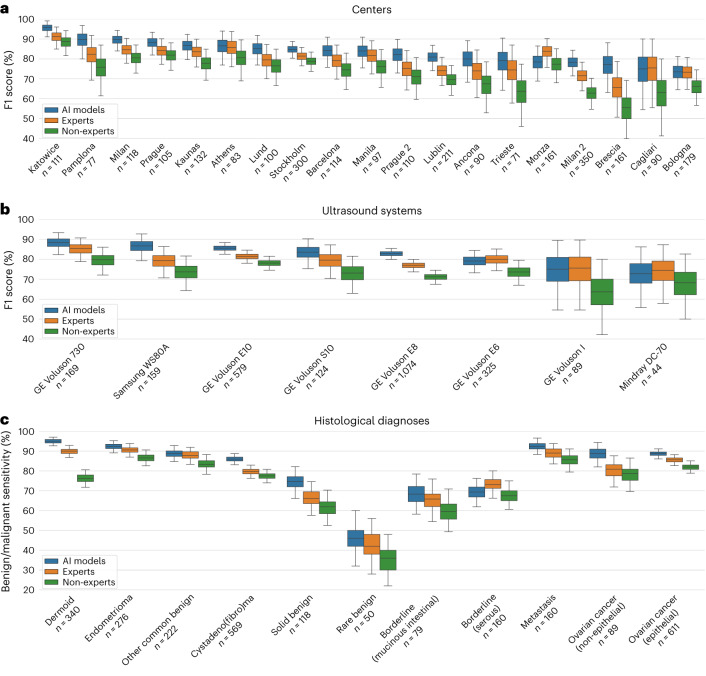
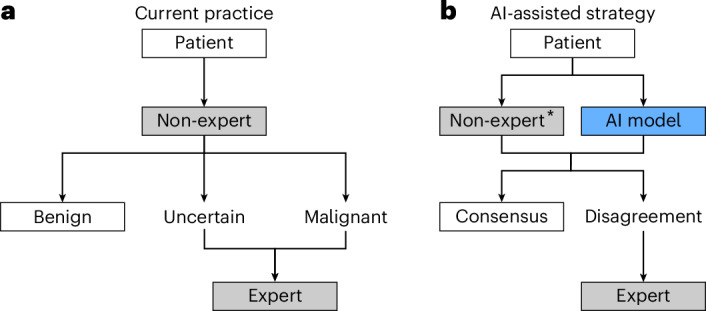
Ovarian lesions are common and often incidentally detected. A critical shortage of expert ultrasound examiners has raised concerns of unnecessary interventions and delayed cancer diagnoses. Deep learning has shown promising results in the detection of ovarian cancer in ultrasound images; however, external validation is lacking. In this international multicenter retrospective study, we developed and validated transformer-based neural network models using a comprehensive dataset of 17,119 ultrasound images from 3,652 patients across 20 centers in eight countries. Using a leave-one-center-out cross-validation scheme, for each center in turn, we trained a model using data from the remaining centers. The models demonstrated robust performance across centers, ultrasound systems, histological diagnoses and patient age groups, significantly outperforming both expert and non-expert examiners on all evaluated metrics, namely F1 score, sensitivity, specificity, accuracy, Cohen's kappa, Matthew's correlation coefficient, diagnostic odds ratio and Youden's J statistic. Furthermore, in a retrospective triage simulation, artificial intelligence (AI)-driven diagnostic support reduced referrals to experts by 63% while significantly surpassing the diagnostic performance of the current practice. These results show that transformer-based models exhibit strong generalization and above human expert-level diagnostic accuracy, with the potential to alleviate the shortage of expert ultrasound examiners and improve patient outcomes.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: E.E., K.S., F.C., E.K. and P.H. have applied for a patent (European patent application 23220765.4) that is pending to a company named Intelligyn. The patent covers methods for a computer-aided diagnostic system to improve generalization and protect against bias. E.E., K.S. and F.C. hold stock in Intelligyn, where E.E. also has an unpaid leadership role. N.C.P.’s institution has received payments for activities not related to this article, including lectures, presentations, expert testimonies, and service on speakers’ bureaus, as well as for travel support. N.C.P. has been an advisory board member of Mindray and GE Healthcare and has held unpaid leadership roles in the POGS Organization of Government Institutions (and the Rizal Medical Service Delivery Network, which are Philippine governmental institutions with the aim to facilitate smooth referral of patients. The other authors declare no competing interests.
Figures






References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
