

The independent and combined associations of nocturnal sleep duration, sleep midpoint, and sleep onset latency with global cognitive function in older Chinese adults
- PMID: 39747731
- PMCID: PMC12181522
- DOI: 10.1007/s11357-024-01476-7
The independent and combined associations of nocturnal sleep duration, sleep midpoint, and sleep onset latency with global cognitive function in older Chinese adults
Abstract
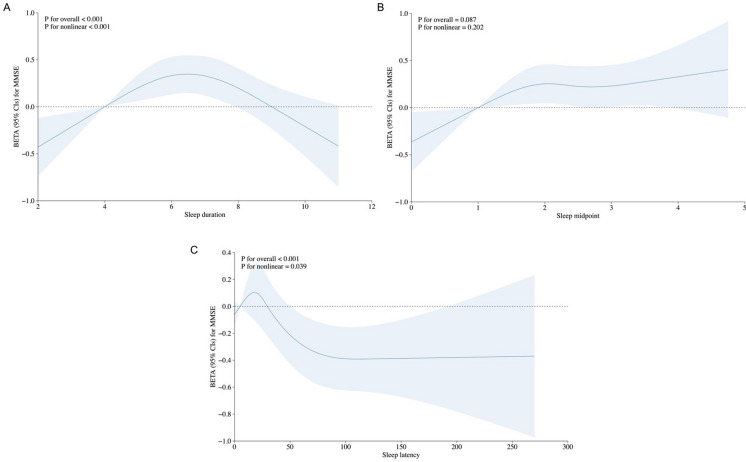
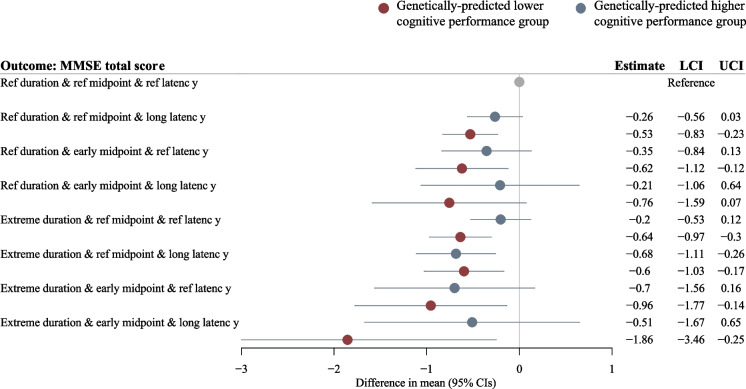
This study aims to investigate the independent and combined associations of nocturnal sleep duration, sleep midpoint, and sleep onset latency with global cognitive function in older Chinese adults. Our cross-sectional study included 4601 community-dwelling cognitively unimpaired adults aged 60 years or older from the West China Health and Aging Cohort Study. Sleep characteristics were assessed using the Pittsburgh Sleep Quality Index, and global cognitive function was evaluated using the Mini-Mental State Examination (MMSE). Multivariable linear regression models were employed, adjusting for an extensive set of demographic, lifestyle, and comorbidity factors. Subgroup analyses were performed based on sex, age, and genetic risk profiles for cognitive performance. The mean age of participants was 69.0 ± 5.53 years, with 52.1% being female. The mean MMSE total score was 24.9 ± 3.20. Compared to the reference category for each sleep variable, sleep duration < 5 h/day or > 8 h/day, sleep midpoint earlier than 1:30 AM, and sleep latency > 60 min were each independently associated with significantly lower MMSE scores (β range - 0.36 to - 0.34; 95% confidence interval range - 0.60 to - 0.10). A combined analysis revealed that individuals with concurrent extreme sleep duration, early midpoint, and/or long latency had even lower MMSE scores, especially among those with genetically predicted poorer cognitive performance (β up to - 1.86). Multiple dimensions of sleep are independently and jointly associated with global cognitive function in older Chinese adults, highlighting the importance of a holistic approach to sleep in cognitive aging research and interventions.
Keywords: Genetic susceptibility; Global cognitive function; Older people; Sleep patterns.
© 2024. The Author(s), under exclusive licence to American Aging Association.
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The research protocol was approved by the Medical Ethics Committee of West China Fourth Hospital of Sichuan University (HXSY-EC-2022034). All participants signed informed consent. The GWAS summary statistics used in the present study are aggregated levels of data which do not contain any personal information. The original GWAS has obtained ethical approval from relevant ethics review committees. Consent for publication: All participants in WCHAC provided consent for publication. Conflict of interest: The authors declare no competing interests.
Figures

References
-
- World Health Organization. Risk reduction of cognitive decline and dementia : WHO guidelines, 78. - PubMed
-
- Kivipelto M, Mangialasche F, Ngandu T. Lifestyle interventions to prevent cognitive impairment, dementia and Alzheimer disease. Nat Rev Neurol. 2018;14(11):653–66. 10.1038/S41582-018-0070-3. - PubMed
-
- Shi L, et al. Sleep disturbances increase the risk of dementia: a systematic review and meta-analysis. Sleep Med Rev. 2018;40:4–16. 10.1016/J.SMRV.2017.06.010. - PubMed
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
