

Development and validation of a real-time prediction model for acute kidney injury in hospitalized patients
- PMID: 39747882
- PMCID: PMC11695981
- DOI: 10.1038/s41467-024-55629-5
Development and validation of a real-time prediction model for acute kidney injury in hospitalized patients
Abstract
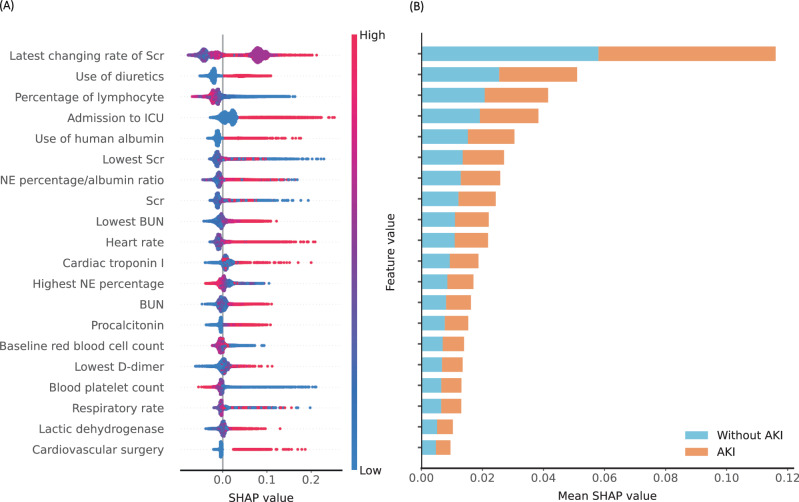
Early prediction of acute kidney injury (AKI) may provide a crucial opportunity for AKI prevention. To date, no prediction model targeting AKI among general hospitalized patients in developing countries has been published. Here we show a simple, real-time, interpretable AKI prediction model for general hospitalized patients developed from a large tertiary hospital in China, which has been validated across five independent, geographically distinct, different tiered hospitals. The model containing 20 readily available variables demonstrates consistent, high levels of predictive discrimination in validation cohort, with AUCs for serum creatinine-based AKI and severe AKI within 48 h ranging from 0.74-0.85 and 0.83-0.90 for transported models and from 0.81-0.90 and 0.88-0.95 for refitted models, respectively. With optimal probability cutoffs, the refitted model could predict AKI at a median of 72 (24-198) hours in advance in internal validation, and 54-90 h in advance in external validation. Broad application of the model in the future may provide an effective, convenient and cost-effective approach for AKI prevention.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests. Inclusion & ethics statement: The research has included local researchers throughout the research process; The research is locally relevant and has been determined in collaboration with local partners; Roles and responsibilities were agreed amongst collaborators ahead of research; This research has not been restricted or prohibited in the setting of the researchers; The study has been approved by all local ethics review committees; The research was undertaken to higher standards of biorisk-related regulations in the local research setting; The research does not result in any risk to participants; We have taken local research relevant to our study into account in citations.
Figures




References
-
- Lameire, N. H. et al. Acute kidney injury: an increasing global concern. Lancet (Lond., Engl.)382, 170–179 (2013). - PubMed
-
- Mehta, R. L. et al. International Society of Nephrology’s 0by25 initiative for acute kidney injury (zero preventable deaths by 2025): a human rights case for nephrology. Lancet (Lond., Engl.)385, 2616–2643 (2015). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
