

New Insights on Continuous Renal Replacement Therapy for Acute Respiratory Distress Syndrome: A Systematic Review and Meta-Analysis
- PMID: 39748202
- PMCID: PMC11695202
- DOI: 10.1111/crj.70045
New Insights on Continuous Renal Replacement Therapy for Acute Respiratory Distress Syndrome: A Systematic Review and Meta-Analysis
Abstract
Background: In recent times, the applications of continuous renal replacement therapy (CRRT) beyond kidney-related conditions have been progressively increasing, and its implementation in randomized controlled trials (RCTs) specifically for acute respiratory distress syndrome (ARDS) has been documented. This meta-analysis compiles all existing RCTs to assess whether CRRT benefits ARDS.
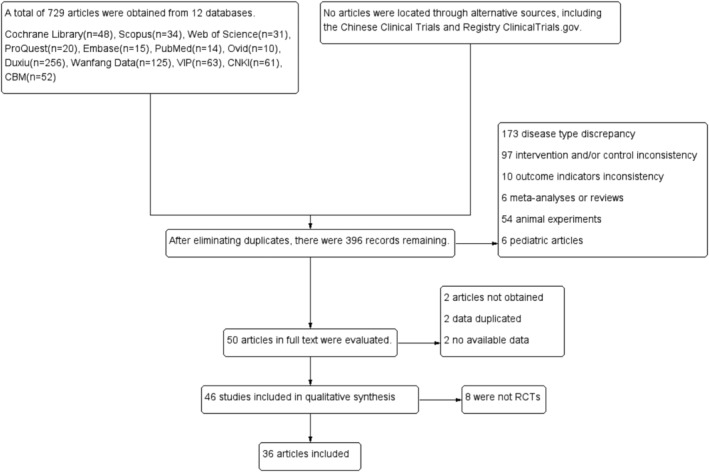
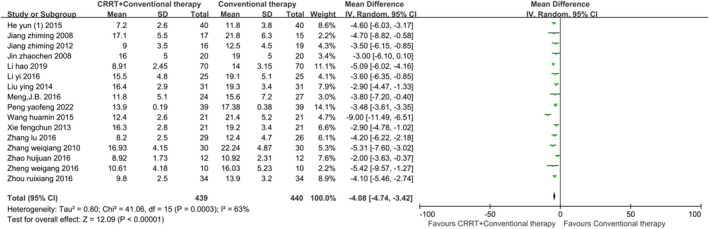
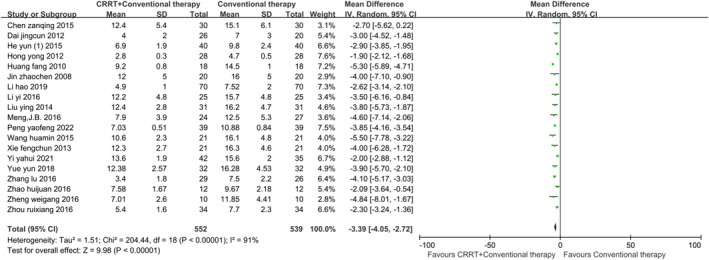
Methods: We searched 12 databases in English and Chinese and two clinical trial centers up to November 28, 2023. The main outcome indicator is the mortality rate. Secondary outcome indicators include incidence of ventilator-associated pneumonia (VAP), ICU length of stay, mechanical ventilation time, oxygenation index (OI) at 24 h (h), OI at 48 h, OI at 72 h, OI at 7 days (d), partial pressure of oxygen (PaO2) at 72 h, Acute Physiology and Chronic Health Evaluation II (APACHE II) score at 24 h, APACHE II score at 48 h, APACHE II score at 72 h, APACHE II score at 7 d, extravascular lung water indexes (EVLWI) at 72 h, TNF-α at 24 h, TNF-α at 7 d, IL-6 at 24 h, IL-6 at 48 h, IL-6 at 72 h, and IL-6 at 7 d. Statistical measures utilized include risk ratios (RR), weighted mean difference (WMD), and 95% confidence intervals (95% CI).
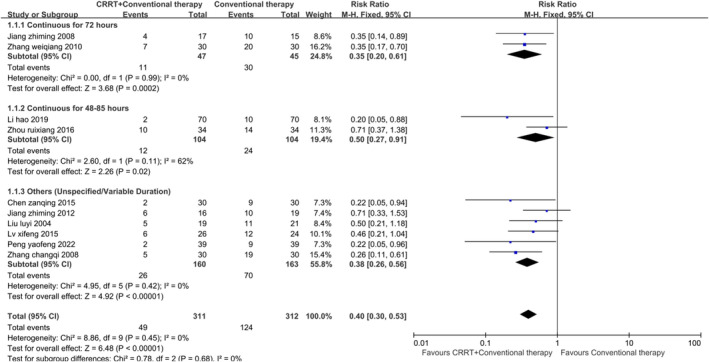
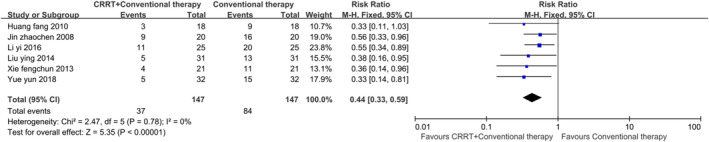
Results: We summarized 36 studies, including 2123 patients. It was found that for ARDS, using CRRT in addition to conventional therapy can reduce the mortality rate (I2 = 0%; RR: 0.40; 95% CI: 0.30-0.53; p < 0.01), the incidence of VAP (I2 = 0%; RR: 0.44; 95% CI: 0.33-0.59; p < 0.01), ICU length of stay, mechanical ventilation time, and EVLWI at 72 h, as well as APACHE II score, TNF-α, and IL-6 at various time points. Additionally, it can increase OI during different time intervals and PaO2 at 72 h.
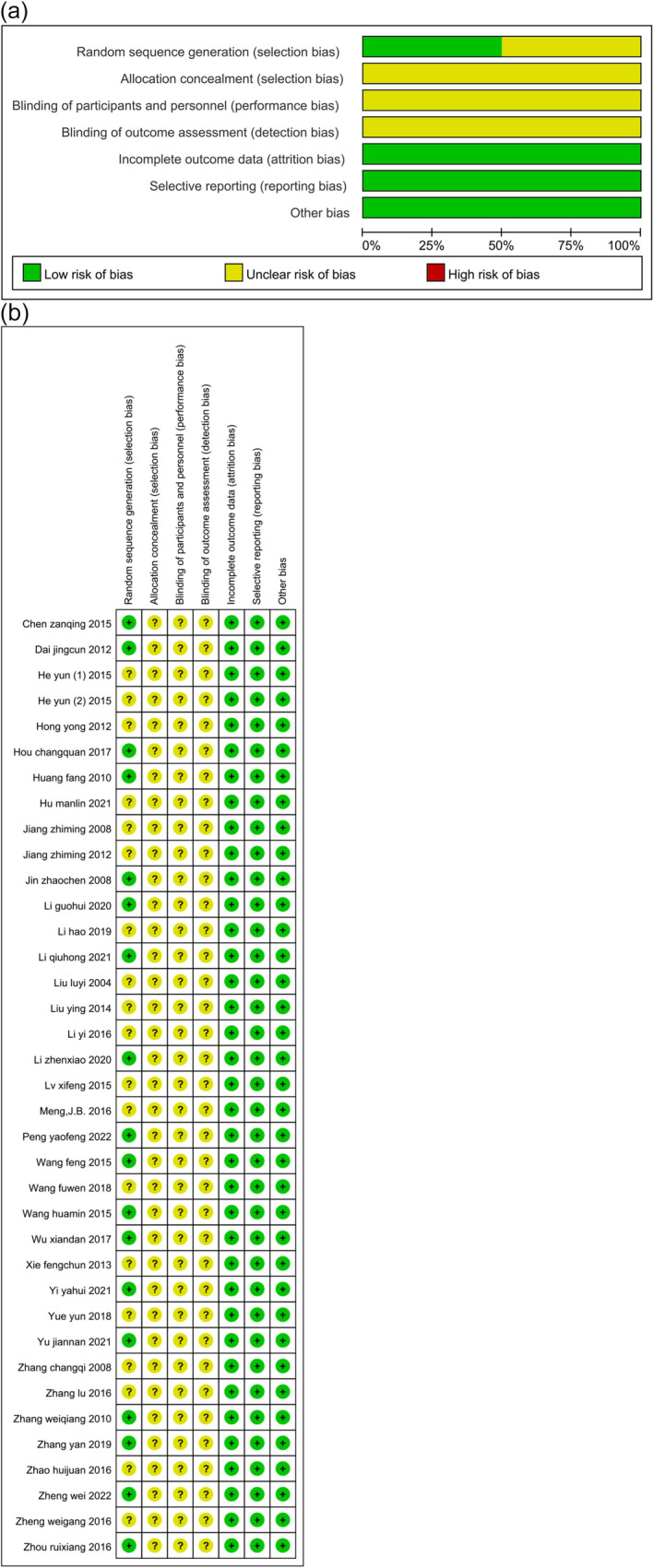
Conclusions: Low-quality evidence suggests that compared with conventional therapy alone, the use of CRRT may be associated with a lower mortality rate, the incidence of VAP, ICU length of stay, mechanical ventilation time, EVLWI, APACHE II score, TNF-α, and IL-6 and may be related to better respiratory function. CRRT may be beneficial for ARDS patients. Future multicenter, well-designed, high-quality RCTs are needed to substantiate these findings.
Keywords: ARDS; CRRT; acute respiratory distress syndrome; continuous renal replacement therapy; meta‐analysis.
© 2025 The Author(s). The Clinical Respiratory Journal published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
- PYQN2023-9/Harbin Medical University Youth Fund
- Z-2018-35-1902/China Foundation for International Medical Exchange
- 82472184/National Natural Science Foundation of China
- JQ2021H002/NSFC Technology Department and Provincial Natural Science Foundation Outstanding Youth Project
- 2021YFC2501800/National Key Research and Development Program of China
LinkOut - more resources
Full Text Sources
