

Preoperative prediction of lymph node metastasis in intrahepatic cholangiocarcinoma: an integrative approach combining ultrasound-based radiomics and inflammation-related markers
- PMID: 39748308
- PMCID: PMC11697736
- DOI: 10.1186/s12880-024-01542-8
Preoperative prediction of lymph node metastasis in intrahepatic cholangiocarcinoma: an integrative approach combining ultrasound-based radiomics and inflammation-related markers
Abstract
Objectives: To develop ultrasound-based radiomics models and a clinical model associated with inflammatory markers for predicting intrahepatic cholangiocarcinoma (ICC) lymph node (LN) metastasis. Both are integrated for enhanced preoperative prediction.
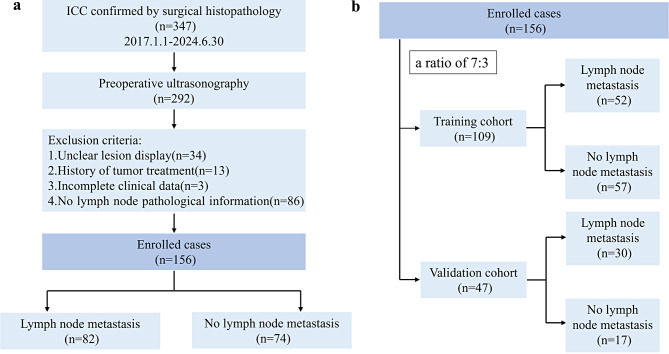
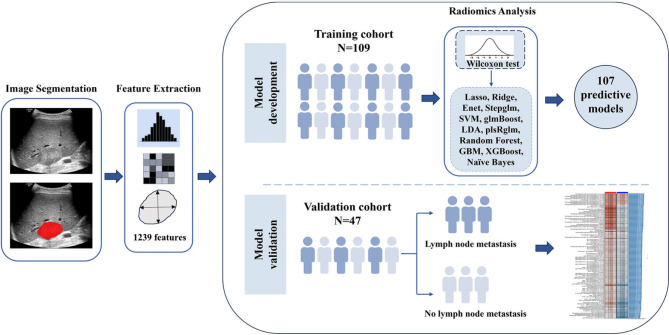
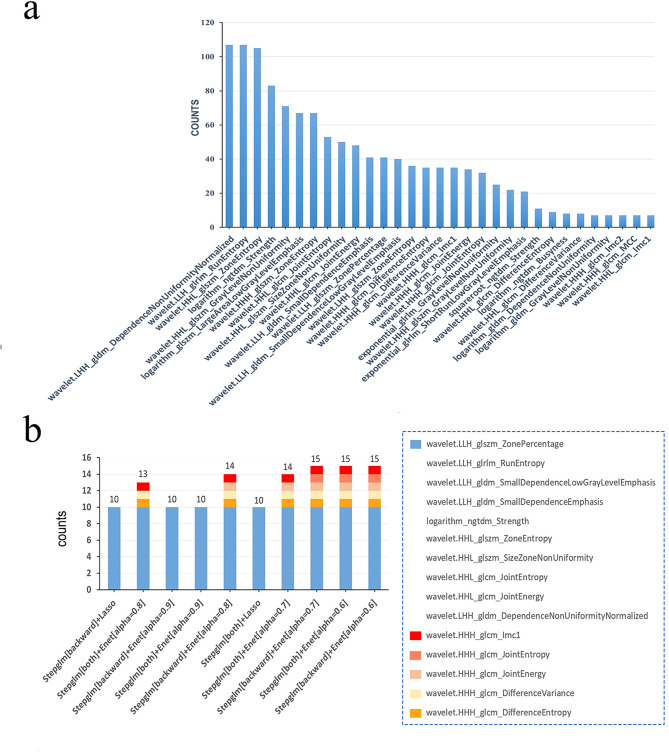
Methods: This study retrospectively enrolled 156 surgically diagnosed ICC patients. A region of interest (ROI) was manually identified on the ultrasound image of the tumor to extract radiomics features. In the training cohort, we performed a Wilcoxon test to screen for differentially expressed features, and then we used 12 machine learning algorithms to develop 107 models within the cross-validation framework and determine the optimal radiomics model through receiver operating characteristic (ROC) curve analysis. Multivariable logistic regression analysis was used to identify independent risk factors to construct a clinical model. The combined model was established by combining ultrasound-based radiomics and clinical parameters. The Delong test and decision curve analysis (DCA) were used to compare the diagnostic efficacy and clinical utility of different models.
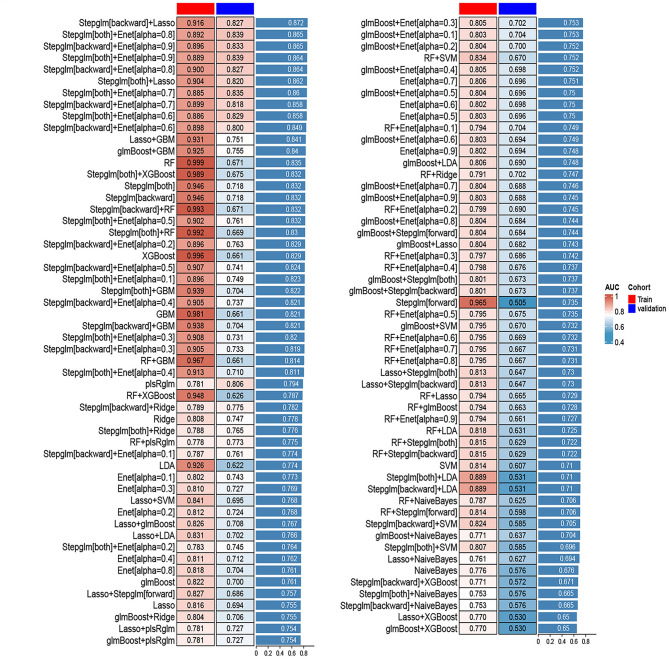
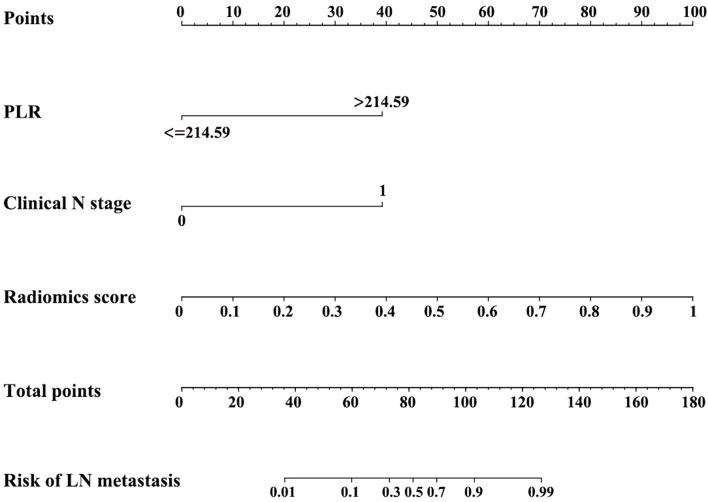
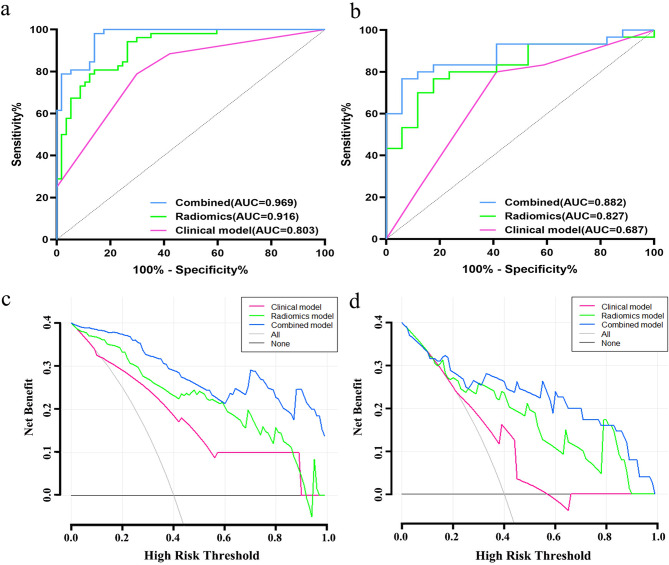
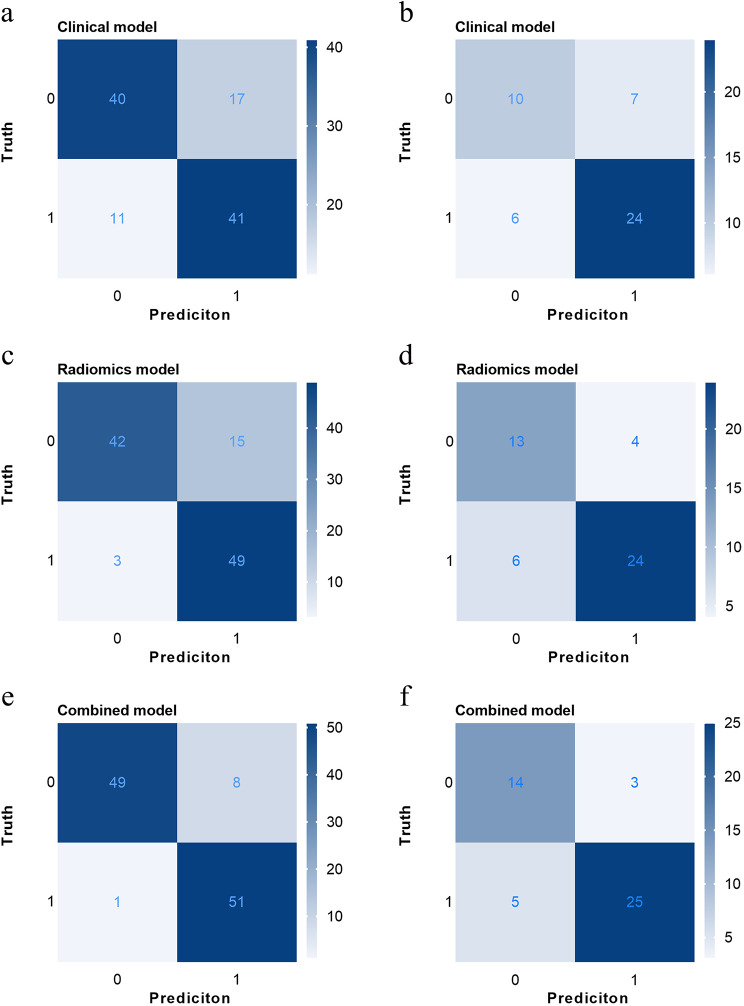
Results: A total of 1239 radiomics features were extracted from the ROIs of tumors. Among the 107 prediction models, the model (Stepglm + LASSO) utilizing 10 radiomics features ultimately yielded the highest average area under the receiver operating characteristic curve (AUC) of 0.872, with an AUC of 0.916 in the training cohort and 0.827 in the validation cohort. The combined model, which incorporates the optimal radiomics score, clinical N stage, and platelet-to-lymphocyte ratio (PLR), achieved an AUC of 0.882 in the validation cohort, significantly outperforming the clinical model with an AUC of 0.687 (P = 0.009). According to the DCA analysis, the combined model also showed better clinical benefits.
Conclusions: The combined model incorporating ultrasound-based radiomics features and the PLR marker offers an effective, noninvasive intelligence-assisted tool for preoperative LN metastasis prediction in ICC patients.
Clinical trial number: Not applicable.
Keywords: Inflammation-related marker; Intrahepatic cholangiocarcinoma; Lymph node metastasis; Radiomics; Ultrasound.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This retrospective study was conducted with approval from the Medical Ethics Committee of First Affiliated Hospital of Guangxi Medical University (No.2024-E421-01). The requirement of informed consent was waived by the Ethics Committee of First Affiliated Hospital of Guangxi Medical University owing to the retrospective nature of the study. Consent for publication: Not applicable. Study subjects or cohorts overlap: 27 study subjects have been previously reported in: Peng YT, Zhou CY, Lin P, et al. Preoperative Ultrasound Radiomics Signatures for Noninvasive Evaluation of Biological Characteristics of Intrahepatic Cholangiocarcinoma. Acad Radiol. 2020;27(6):785–797. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Machine learning-based Radiomics analysis for differentiation degree and lymphatic node metastasis of extrahepatic cholangiocarcinoma.BMC Cancer. 2021 Nov 24;21(1):1268. doi: 10.1186/s12885-021-08947-6. BMC Cancer. 2021. PMID: 34819043 Free PMC article.
-
Radiomics using CT images for preoperative prediction of lymph node metastasis in perihilar cholangiocarcinoma: a multi-centric study.Eur Radiol. 2024 Feb;34(2):1280-1291. doi: 10.1007/s00330-023-10108-1. Epub 2023 Aug 17. Eur Radiol. 2024. PMID: 37589900
-
To accurately predict lymph node metastasis in patients with mass-forming intrahepatic cholangiocarcinoma by using CT radiomics features of tumor habitat subregions.Cancer Imaging. 2025 Feb 26;25(1):19. doi: 10.1186/s40644-025-00842-8. Cancer Imaging. 2025. PMID: 40011960 Free PMC article.
-
The Application Status of Radiomics-Based Machine Learning in Intrahepatic Cholangiocarcinoma: Systematic Review and Meta-Analysis.J Med Internet Res. 2025 May 5;27:e69906. doi: 10.2196/69906. J Med Internet Res. 2025. PMID: 40323647 Free PMC article. Review.
-
Artificial Intelligence and Radiomics in Cholangiocarcinoma: A Comprehensive Review.Diagnostics (Basel). 2025 Jan 10;15(2):148. doi: 10.3390/diagnostics15020148. Diagnostics (Basel). 2025. PMID: 39857033 Free PMC article. Review.
References
-
- Valle JW, Kelley RK, Nervi B, Oh DY, Zhu AX. Biliary tract cancer. Lancet. 2021;397(10272):428–44. - PubMed
-
- Mazzaferro V, Gorgen A, Roayaie S, Droz Dit Busset M, Sapisochin G. Liver resection and transplantation for intrahepatic cholangiocarcinoma. J Hepatol. 2020;72(2):364–77. - PubMed
-
- Navarro JG, Lee JH, Kang I, et al. Prognostic significance of and risk prediction model for lymph node metastasis in resectable intrahepatic cholangiocarcinoma: do all require lymph node dissection? HPB (Oxford). 2020;22(10):1411–9. - PubMed
-
- Bridgewater J, Galle PR, Khan SA, et al. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J Hepatol. 2014;60(6):1268–89. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
