

Sepsis-induced cardiogenic shock: controversies and evidence gaps in diagnosis and management
- PMID: 39748440
- PMCID: PMC11694368
- DOI: 10.1186/s40560-024-00770-y
Sepsis-induced cardiogenic shock: controversies and evidence gaps in diagnosis and management
Abstract
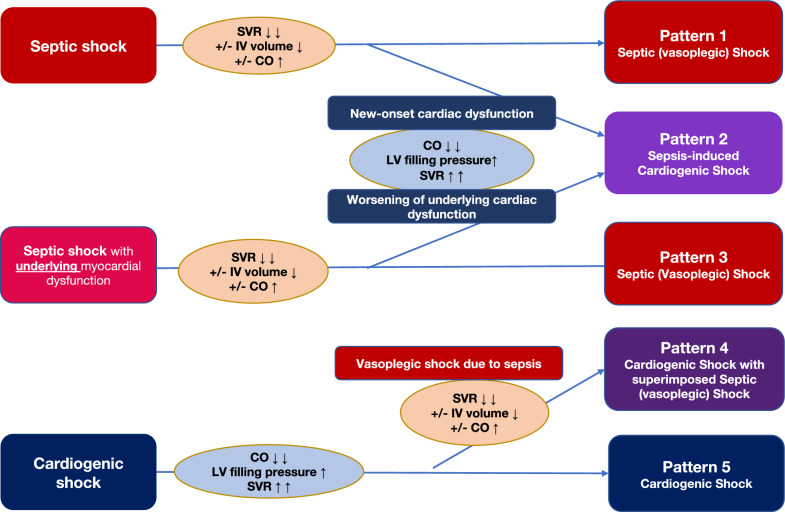
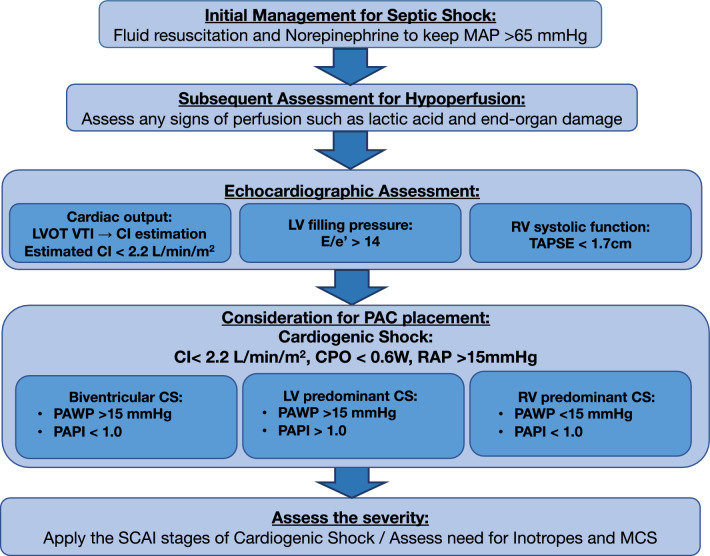
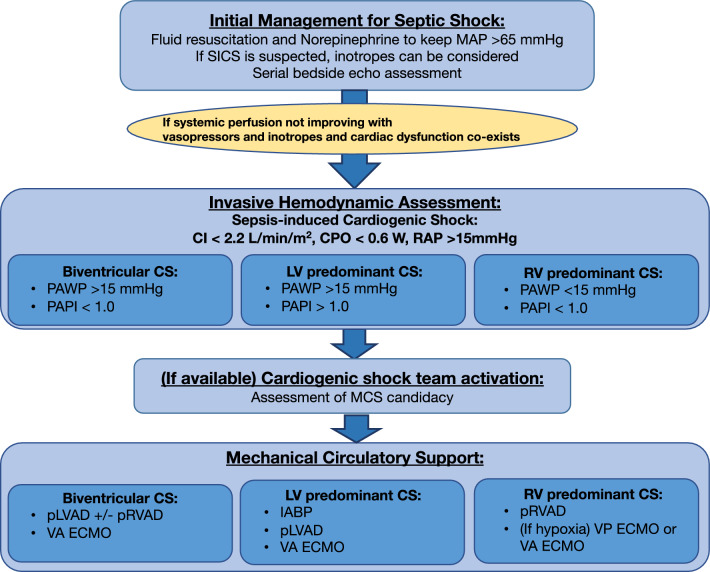
Sepsis often leads to vasoplegia and a hyperdynamic cardiac state, with treatment focused on restoring vascular tone. However, sepsis can also cause reversible myocardial dysfunction, particularly in the elderly with pre-existing heart conditions. The Surviving Sepsis Campaign Guidelines recommend using dobutamine with norepinephrine or epinephrine alone for patients with septic shock with cardiac dysfunction and persistent hypoperfusion despite adequate fluid resuscitation and stable blood pressure. However, the definition of cardiac dysfunction and hypoperfusion in these guidelines remains controversial, leading to varied clinical interpretations. Cardiac dysfunction with persistent hypoperfusion despite restoring adequate preload and afterload is often considered a cardiogenic shock. Therefore, sepsis complicated by new-onset myocardial dysfunction or worsening of underlying myocardial dysfunction due to sepsis-induced cardiomyopathy, resulting in cardiogenic shock, can be defined as "Sepsis-induced cardiogenic shock (SICS)". SICS is known to be associated with significantly higher mortality. A history of cardiac dysfunction is a strong predictor of SICS, highlighting the need for precise diagnosis and management given the aging population and rising cardiovascular disease prevalence. Therefore, SICS might benefit from early invasive hemodynamic monitoring with a pulmonary artery catheter (PAC), unlike those with septic shock alone. While routine PAC monitoring for all septic patients is impractical, echocardiography could be a useful screening tool for high-risk individuals. If echocardiography indicates cardiogenic shock, PAC might be warranted for continuous monitoring. The role of inotropes in SICS remains uncertain. Mechanical circulatory support (MCS) might be considered for severe cases, as high-dose vasopressors and inotropes are associated with worse outcomes. Correct patient selection is the key to improving outcomes with MCS. Engaging a cardiogenic shock team for a multidisciplinary approach can be beneficial. In summary, addressing the evidence gaps in SICS diagnosis and management is crucial. Echocardiography for screening, advanced monitoring with PAC, and careful patient selection for MCS are important for optimal patient care.
Keywords: Cardiogenic shock; Mechanical circulatory support; Mixed shock; Sepsis-induced cardiomyopathy; Septic cardiomyopathy; Septic shock.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: None.
Figures
References
-
- Hochman JS, Sleeper LA, Webb JG, Sanborn TA, White HD, Talley JD, Buller CE, Jacobs AK, Slater JN, Col J, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should we emergently revascularize occluded coronaries for cardiogenic shock. N Engl J Med. 1999;341(9):625–34. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
