

The Usefulness of Mandibular Anglectomy in Patients With Masticatory Muscle Tendon-Aponeurosis Hyperplasia: A Preliminary Single-Center Survey
- PMID: 39749059
- PMCID: PMC11695028
- DOI: 10.7759/cureus.74994
The Usefulness of Mandibular Anglectomy in Patients With Masticatory Muscle Tendon-Aponeurosis Hyperplasia: A Preliminary Single-Center Survey
Abstract
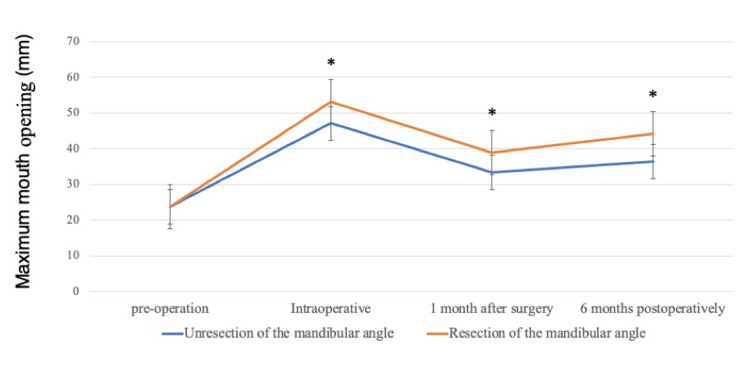
Objective Masticatory muscle tendon-aponeurosis hyperplasia (MMTAH) is a recently identified condition characterized by restricted mouth opening due to hyperplasia of the temporalis muscle tendon and masseter muscle aponeurosis. This study examines the treatment and clinical course of patients with MMTAH who underwent surgery at our hospital. Subjects and methods The study included 14 patients (four males and 10 females; mean age: 33.9 years; age range: 17-50 years) who were clinically diagnosed with MMTAH at our hospital between 2008 and 2020. The surgical procedure, as well as the preoperative, intraoperative, and postoperative mouth opening range of each patient, were examined. Results In all cases, the mouth opening range significantly improved postoperatively. Patients who underwent mandibular anglectomy showed a significantly greater mouth opening range both preoperatively and postoperatively compared to those who did not undergo the procedure. Additionally, mandibular anglectomy was effective in maintaining the mouth opening range at six months in patients who underwent the procedure, in contrast to those who did not. Conclusions Mandibular anglectomy appears to be effective in maintaining the mouth opening range in patients with MMTAH. While additional case studies are needed to confirm our findings, we believe that mandibular anglectomy is a valuable treatment option for MMTAH.
Keywords: anglectomy; masticatory muscle tendon-aponeurosis hyperplasia; mmtah; square mandible; trisumus.
Copyright © 2024, Yoshiga et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. The Kyushu Dental University Hospital Ethics Committee issued approval 23-28. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- Trismus: aetiology, differential diagnosis and treatment. Dhanrajani PJ, Jonaidel O. Dent Update. 2002;29:88-92, 94. - PubMed
-
- Bruxism and hypertrophy of the masseter muscle: a clinical, morphological and functional investigation. Ahlgren J, Omnell KA, Sonesson B, Toremalm NG. Pract Otorhinolaryngol (Basel) 1969;31:22–29. - PubMed
LinkOut - more resources
Full Text Sources