

Phenotype Spectrum of TRPM3-Associated Disorders
- PMID: 39749750
- PMCID: PMC11831877
- DOI: 10.1002/ana.27141
Phenotype Spectrum of TRPM3-Associated Disorders
Abstract
Objective: Monoallelic variants in the transient receptor potential melastatin-related type 3 gene (TRPM3) have been associated with neurodevelopmental manifestations, but knowledge on the clinical manifestations and treatment options is limited. We characterized the clinical spectrum, highlighting particularly the epilepsy phenotype, and the effect of treatments.
Methods: We analyzed retrospectively the phenotypes and genotypes of 43 individuals with TRPM3 variants, acquired from GeneMatcher and collaborations (n = 21), and through a systematic literature search (n = 22). We included all patients with a pathogenic TRPM3 variant.
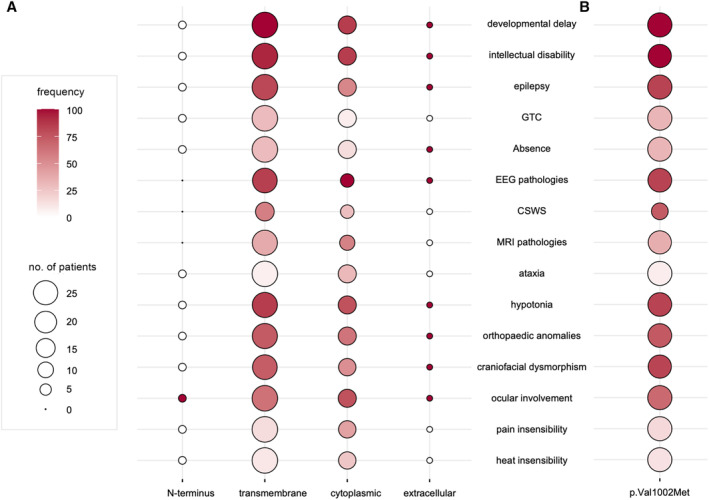
Results: The median age at the time of the study was 10 years, with a preponderance of girls (60%) versus boys (40%). Frequent findings were developmental delay and/or intellectual disability (93%), global or axial hypotonia (77%), ocular involvement (70%), musculoskeletal anomalies (65%), and dysmorphic features (58%). Epilepsy was diagnosed in 31 patients (72%), classified in all as developmental and epileptic encephalopathy with or without spike wave activation in sleep (DEE/DEE-SWAS). Patients with the variant p.Val1002Met (n = 24) significantly more often had developmental delay and epilepsy. The most effective anti-seizure medication was primidone. All treated patients showed an improvement in seizure frequency, motor and speech development, and/or learning capability with this drug.
Interpretation: Developmental delay/intellectual disability and epilepsy are dominant phenotypic features in patients with TRPM3 variants. Given that epilepsy can negatively impact development, screening for awake and sleep electroencephalogram abnormalities and other manifestations are essential to offer early intervention. The TRPM3 channel blocker primidone has shown promising effects and should be considered in every child with a TRPM3 gain-of-function variant. ANN NEUROL 2025;97:561-570.
© 2025 The Author(s). Annals of Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
Nothing to report.
Figures


References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
