

First-line immune-based combinations or sunitinib in favorable-risk metastatic renal cell carcinoma: a real-world retrospective comparison from the ARON-1 study
- PMID: 39752009
- PMCID: PMC11699065
- DOI: 10.1007/s00262-024-03897-x
First-line immune-based combinations or sunitinib in favorable-risk metastatic renal cell carcinoma: a real-world retrospective comparison from the ARON-1 study
Abstract
Introduction: Renal cell carcinoma (RCC) is one of the most common types of urogenital cancer. The introduction of immune-based combinations, including dual immune-checkpoint inhibitors (ICI) or ICI plus tyrosine kinase inhibitors (TKIs), has radically changed the treatment landscape for metastatic RCC, showing varying efficacy across different prognostic groups based on the International Metastatic RCC Database Consortium (IMDC) criteria.
Materials and methods: This retrospective multicenter study, part of the ARON-1 project, aimed to evaluate the outcomes of favorable-risk metastatic RCC patients treated with immune-based combinations or sunitinib. Patients were assessed for overall survival (OS), progression-free survival (PFS) and overall response rate. We carried out a survival analysis by a Cox regression model.
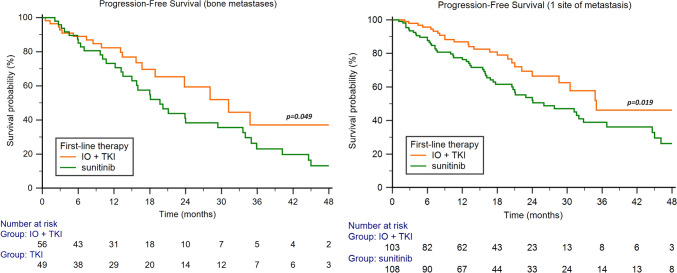
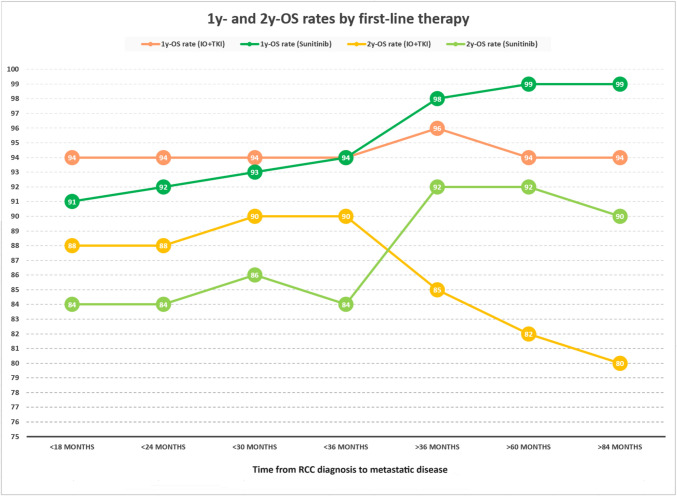
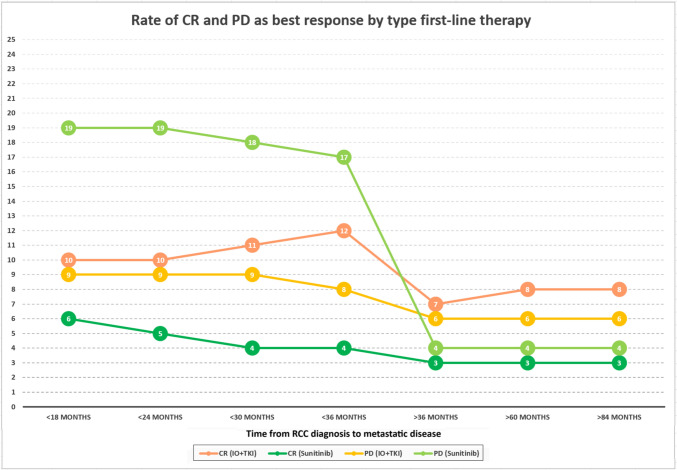
Results: A total of 524 favorable-risk patients were included in the analysis. After a median follow-up of 37.2 months, the median OS in the overall population was 56.1 months. There was no significant difference in OS between patients receiving sunitinib and those receiving TKI + ICI combinations (p = 0.761). Patients on TKI + ICI had significantly longer PFS compared to patient treated with sunitinib (30.7 vs 22.9 months, p = 0.007). Analysis of OS and PFS based on metastatic site revealed that patients with bone metastases benefited more from ICI plus TKI (56 patients with bone metastases receiving IO + TKI, 38 received pembrolizumab plus axitinib, 15 cabozantinib plus nivolumab and 3 pembrolizumab plus lenvatinib), while sunitinib was more effective for pancreatic and glandular metastases. Additionally, the number of metastatic sites played a role, with TKI plus ICI showing superiority in patients with a single metastatic site. The time from RCC diagnosis to metastatic disease also impacted outcomes, with TKI plus ICI being more effective in patients with a shorter interval (i.e., < 36 months).
Conclusions: The choice between upfront combination or monotherapy for metastatic favorable prognosis RCC remains a current issue. While combination therapy offers prolonged PFS, it does not necessarily translate to improve OS compared to sunitinib. This real-world study supports the superiority in terms of PFS of TKI plus ICI vs TKI monotherapy but not in OS. Probable, other clinical factors should be taking into account to make clinical treatment decisions in this setting.
Keywords: ARON-1 study; Good favorable-risk IMDC criteria; Immune-based combinations; Immunotherapy; Renal cell carcinoma.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflicts of Interest: Javier Molina-Cerrillo declares consultant, advisory or speaker roles for IPSEN, Roche, Pfizer, Sanofi, Janssen and BMS. JMC has received research grants from Pfizer, IPSEN and Roche Francesco Massari has received research support and/or honoraria from Astellas, BMS, Janssen, Ipsen, MSD and Pfizer outside the submitted work. Linda Cerbone has received honoraria for advisory boards, speaker engagements and scientific consultancy for educational purposes from AstraZeneca, EISAI, MSD, Ipsen, BMS, A.A.A.; past MSD employee in Medical Affairs. Ondrej Fiala received honoraria from Novartis, Janssen, Merck and Pfizer for consultations and lectures unrelated to this project. Fernando Sabino M. Monteiro has received research support from Janssen, Merck Sharp Dome and honoraria from Janssen, Ipsen, Bristol Myers Squibb and Merck Sharp Dome, all unrelated to the present paper. R. Kanesvaran has received fees for speaker bureau and advisory board activities from the following companies; Pfizer, MSD, BMS, Eisai, Ipsen, Johnson and Johnson, Merck, Amgen, Astellas and Bayer. Camillo Porta has received honoraria from Angelini Pharma, AstraZeneca, BMS, Eisai, Ipsen and MSD and acted as a Protocol Steering Committee Member for BMS, Eisai and MSD. Sebastiano Buti has received honoraria for speaking at scientific events and advisory roles from AstraZeneca, Bristol Myers Squibb, Ipsen, Merck, Eisai, MSD, Novartis and Pfizer and research funding from Novartis and Pfizer. Matteo Santoni has received research support and honoraria from Janssen, Bristol Myers Squibb, Ipsen, MSD, Astellas, A.A.A. and Bayer, all unrelated to the present paper. The other authors declare no conflicts of interest.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
