

Rurality predisposes departure from gold-standard care, leading to delayed or accelerated access to surgery: insights from a scoping review
- PMID: 39753325
- PMCID: PMC11684926
- DOI: 10.1503/cjs.000124
Rurality predisposes departure from gold-standard care, leading to delayed or accelerated access to surgery: insights from a scoping review
Abstract
Background: Because tertiary centres are generally situated at urban sites, it is unclear whether patients in rural areas have the same access to surgical services that patients in urban areas do. We sought to map the North American evidence landscape of how rurality affects access to medically indicated surgeries and identify system-, patient-, and provider-level barriers that preclude urban-comparable care.
Methods: We carried out a systematic search adhering to PRISMA for Scoping Reviews methodology across PubMed, MEDLINE, Scopus, and Web of Science, encompassing literature from the last 26 years (January 2023). Search terms included "rural population," "health care access," "surgical procedures," and "health disparities." We synthesized our findings using a narrative approach.
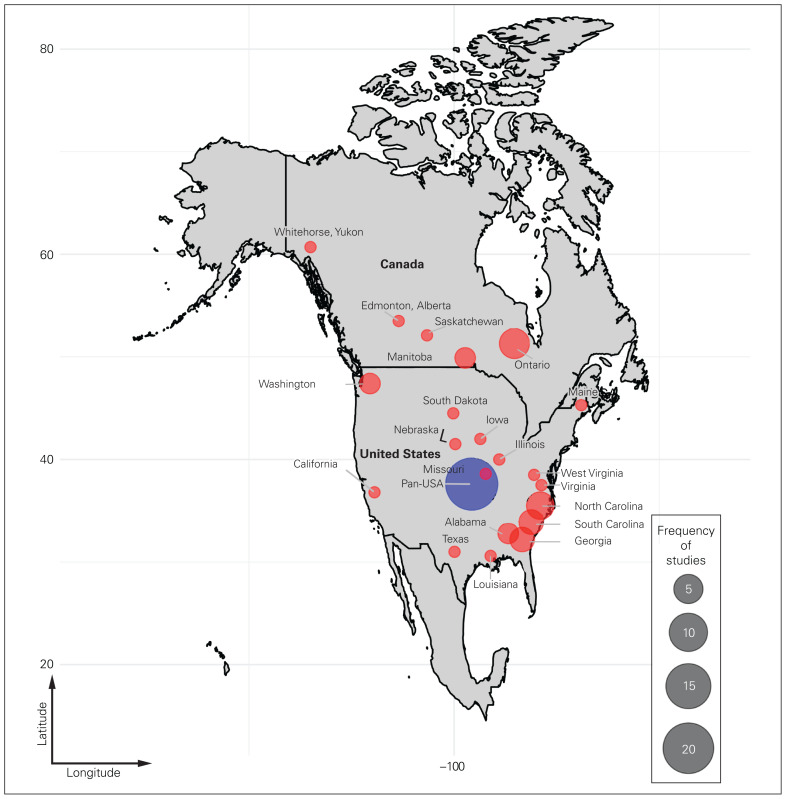
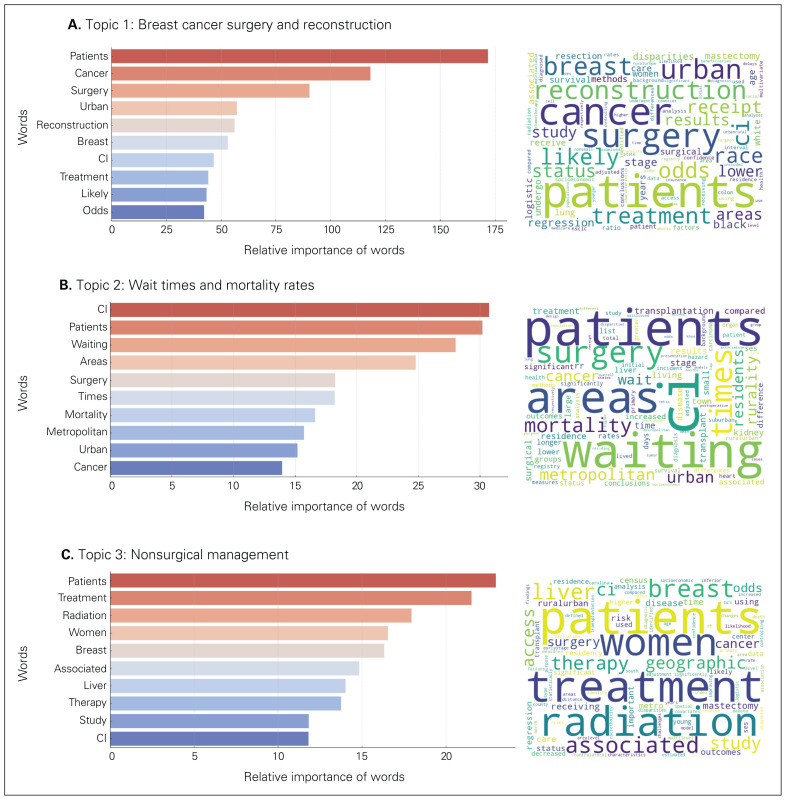
Results: Of 13 897 identified studies, we included 71 publications, spanning a wide spectrum of surgical disciplines. Of these, 83% reported diminished and 17% reported accelerated access to surgery, and 30% reported an interaction between rurality with other social determinants of health, particularly age, sex and gender, and race and ethnicity. Of the studies that reported diminished access, top cited reasons included primary and specialist provider density, differences in patients' socioeconomic profiles, and provision of comparable counselling during surgical decisionmaking. Strikingly, a key driver of enhanced surgical access was an absence of specialized medical interventions leading to an overreliance on surgical alternatives.
Conclusion: Whether surgical access was diminished or accelerated, the net impact of rurality was a deviation from guideline-concordant care. A key implication of these findings is that reliance on surgical wait times alone can skew perception of surgical access, advocating for adoption of integrated quality-of-care metrics that better reflect access to comprehensive medical and surgical treatment programs.
Contexte: Étant donné que les centres de soins tertiaires se trouvent généralement en milieu urbain, on peut se demander si l'accès aux services chirurgicaux est le même en région rurale qu'en milieu urbain. Nous avons voulu cartographier, preuve à l'appui, l'impact de la ruralité sur l'accès à des chirurgies médicalement indiquées en Amérique du Nord et identifier les obstacles, propres au système, à la patientèle et aux équipes soignantes, qui nuisent à la prestation des soins équivalents à ceux des milieux urbains. MÉTHODES: Nous avons procédé à une interrogation systématique (conforme à la Norme de réalisation de revue systématique de la littérature PRISMA) des bases de données PubMed, MEDLINE, Scopus et Web of Science regroupant la littérature des 26 dernières années (janvier 2023). Les mots clés de langue anglaise utilisés incluaient : « rural population », « health care access », « surgical procedures » et « health disparities ». Nous avons synthétisé nos observations au moyen d'une approche narrative. RÉSULTATS: Des 13 897 études recensées, nous avons retenu 71 publications abordant un vaste éventail de disciplines chirurgicales. Parmi ces publications, 83 % faisaient état d'un accès diminué, 17 % d'un accès plus rapide à la chirurgie, et 30 % d'un lien entre la ruralité et d'autres déterminants sociaux de la santé, notamment l'âge, le sexe et le genre, ainsi que la race et l'ethnicité. Selon les études ayant fait état d'un accès diminué, les principales raisons incluaient la densité des effectifs en médecine primaire et de spécialité, les différences de profils socioéconomiques de la patientèle et l'offre d'un counselling comparable lors du processus décisionnel concernant la chirurgie. À noter, l'un des principaux facteurs d'amélioration de l'accès aux soins chirurgicaux était l'absence d'interventions médicales spécialisées associées à une dépendance indue à l'endroit des solutions chirurgicales.
Conclusion: Que l'accès à la chirurgie ait été diminué ou accéléré, l'impact net de la ruralité a pris la forme d'un écart par rapport aux soins préconisés par les lignes directrices. Ces observations indiquent principalement que la dépendance à l'égard des temps d'attente en chirurgie seule peut fausser la perception quant à l'accès aux soins chirurgicaux, ce qui milite en faveur de l'adoption de paramètres de qualité de soins intégrés qui reflèteraient plus fidèlement l'accès à des programmes de traitements médicaux et chirurgicaux complets.
© 2025 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests:: Alisha Ebrahim, Sarthak Sinha, Ifeoluwa Adedipe, and Abeer Ahmad acknowledge the support of the Department of Distributed Learning and Rural Initiatives, Cumming School of Medicine, University of Calgary (not paid to authors). Aaron Johnston reports receiving travel support from the College of Family Physicians of Canada (CFPC). Dr. Johnston also holds volunteer roles with CFPC and the Association of Faculties of Medicine of Canada. No other competing interests were declared.
Figures

Similar articles
-
Rural-urban differences in wait-time to general surgical outpatient care.Can J Rural Med. 2025 Apr 1;30(2):89-95. doi: 10.4103/cjrm.cjrm_12_24. Epub 2025 May 20. Can J Rural Med. 2025. PMID: 40366288 English, French.
-
N° 367-2019 Lignes Directrices Canadiennes Sur L'activité Physique Durant La Grossesse.J Obstet Gynaecol Can. 2018 Nov;40(11):1538-1548. doi: 10.1016/j.jogc.2018.09.003. Epub 2018 Oct 18. J Obstet Gynaecol Can. 2018. PMID: 30343980
-
No 385 - Indications de l'examen pelvien.J Obstet Gynaecol Can. 2019 Aug;41(8):1235-1250. doi: 10.1016/j.jogc.2019.04.003. J Obstet Gynaecol Can. 2019. PMID: 31331611
-
Factors influencing retention of International Medical Graduates in rural practice.Can J Rural Med. 2025 Jan 1;30(1):17-30. doi: 10.4103/cjrm.cjrm_6_24. Epub 2025 Mar 11. Can J Rural Med. 2025. PMID: 40052776 Review. English, French.
-
In situ clinical education of frontline healthcare providers in under-resourced areas: A rapid review.Can J Rural Med. 2024 Jan 1;29(1):20-29. doi: 10.4103/cjrm.cjrm_95_22. Epub 2024 Feb 20. Can J Rural Med. 2024. PMID: 38372264 Review. English, French.
Cited by
-
Twelve Tips for Engaging Medical Students in Rural-Focused Research.MedEdPublish (2016). 2025 May 16;14:243. doi: 10.12688/mep.20642.3. eCollection 2024. MedEdPublish (2016). 2025. PMID: 39931306 Free PMC article.
References
-
- Berini CR, Bonilha HS, Simpson AN. Impact of community health workers on access to care for rural populations in the United States: a systematic review. J Community Health 2022;47:539–53. - PubMed
-
- Caron NR, Pinney SJ. Surgery in rural Canada: challenges and possible solutions. In: Wichmann M, Borgstrom D, Caron N, et al.. editors. Rural surgery. Berlin: Springer Berlin Heidelberg; 2011:7–14.
-
- Kozhimannil KB, Henning-Smith C. Improving health among rural residents in the US. JAMA 2021;325:1033. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials