

Risk factors for bloodstream infection in COVID-19 patients in intensive care units: a systematic review and meta-analysis
- PMID: 39754037
- PMCID: PMC11697680
- DOI: 10.1186/s12879-024-10420-1
Risk factors for bloodstream infection in COVID-19 patients in intensive care units: a systematic review and meta-analysis
Abstract
Background: Risk factors for bloodstream infection in patients with COVID-19 in the intensive care unit (ICU) remain unclear. The purpose of this systematic review was to study the risk factors for BSI in patients admitted to ICUs for COVID-19.
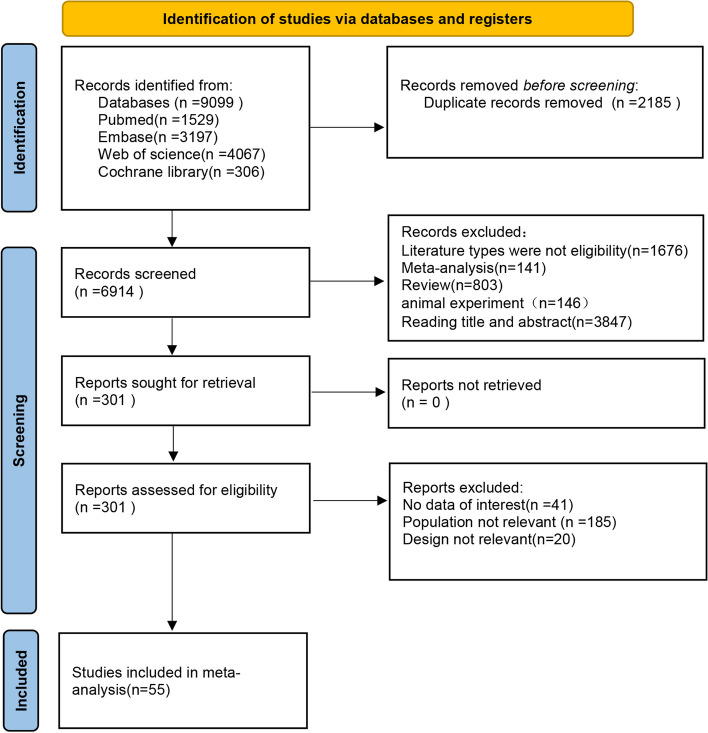
Methods: A systematic search was performed on PubMed, EMBASE, Cochrane Library, and Web of Science up to July 2024. Data were reported as combined odds ratio (OR) for categorical variables and weighted mean difference (WMD) for continuous variables.
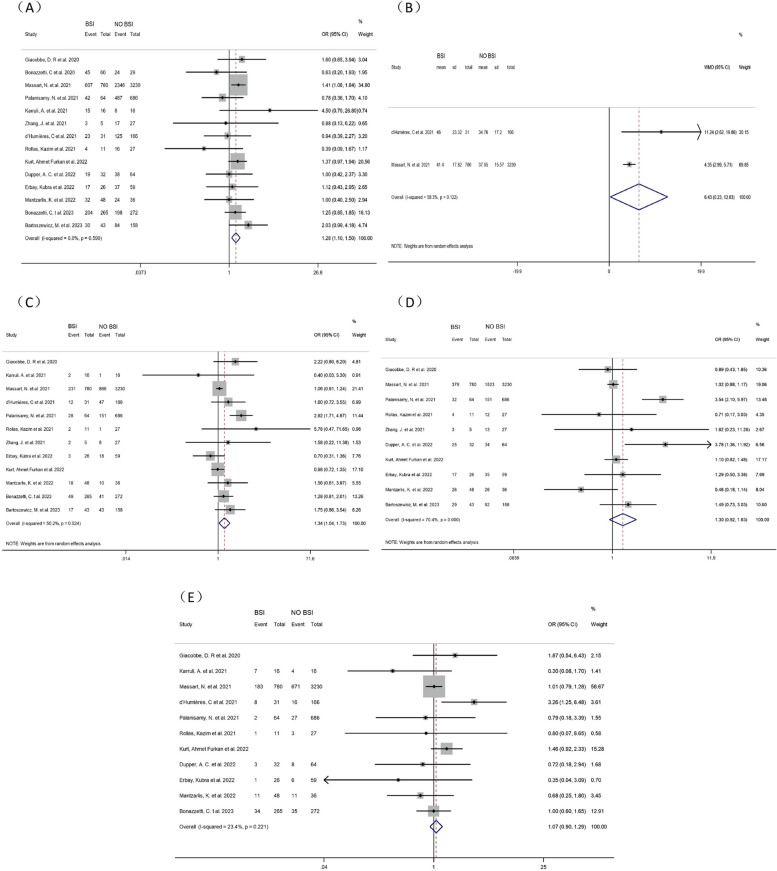
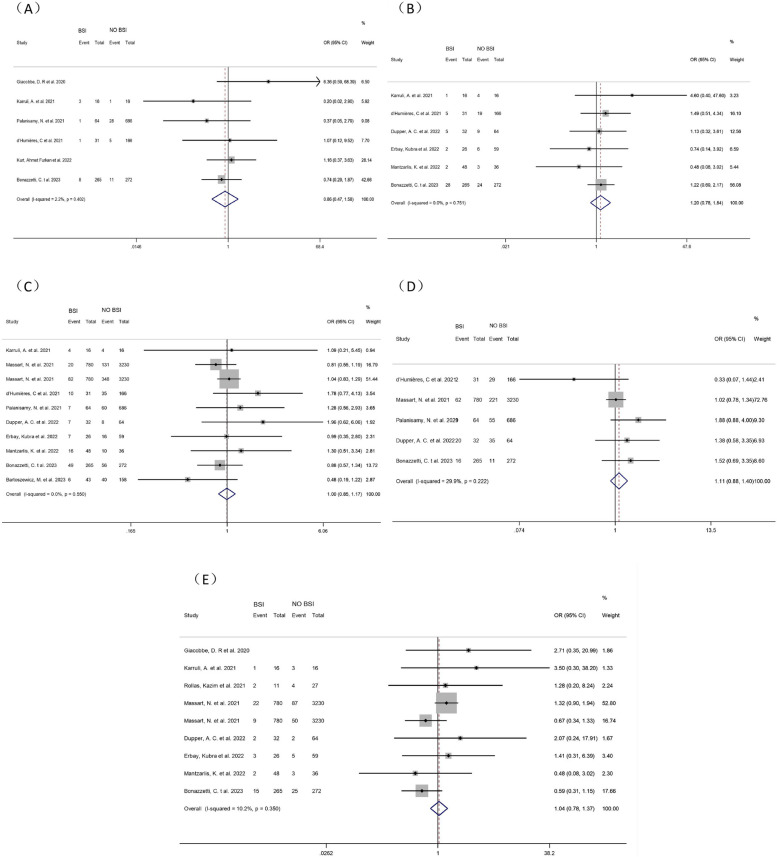
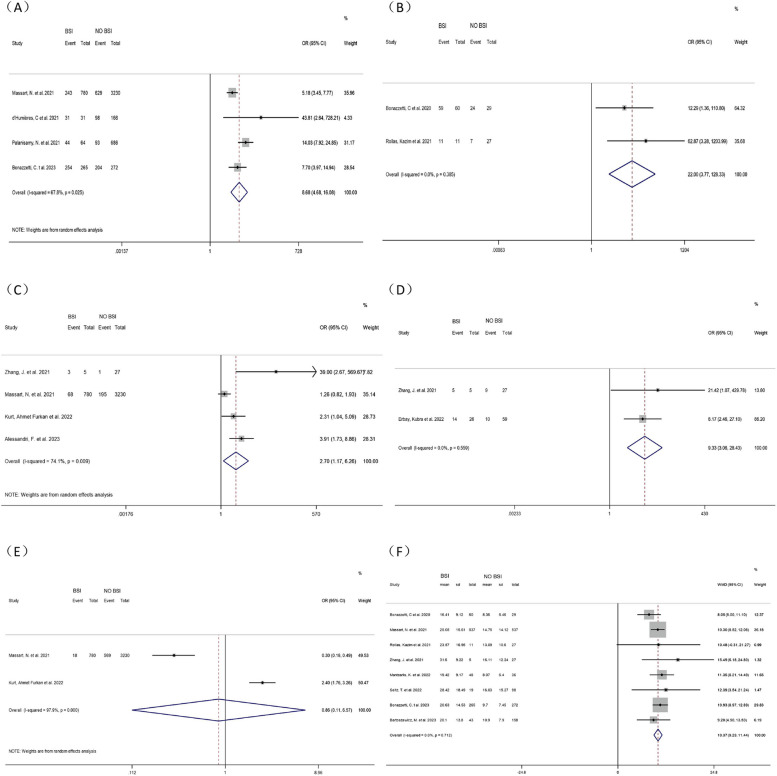
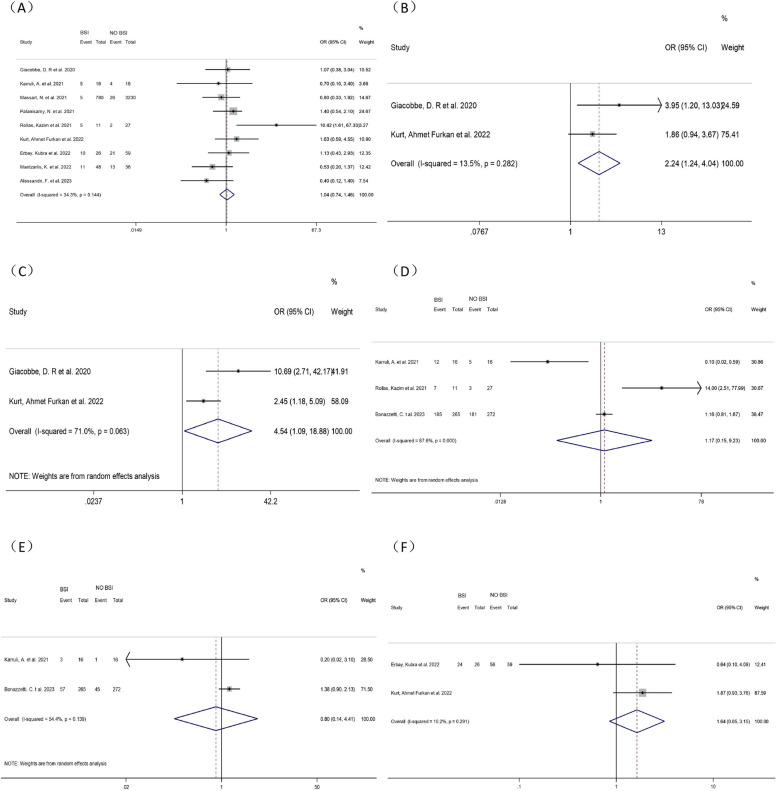
Results: 6914 studies were retrieved, of which 55 were included in the meta-analysis. Men (OR = 1.28, 95% CI: 1.10-1.50, P = 0.006), high SAPS II score (WMD = 6.43, 95% CI: 0.23-12.63, P = 0.042), diabetes (OR = 1.34, 95% CI: 1.04-1.73, P = 0.022), tracheal intubation (OR = 8.68, 95% CI: 4.68-16.08, P < 0.001), mechanical ventilation (OR = 22.00, 95% CI: 3.77-128.328, P < 0.001), ECMO (OR = 2.70, 95% CI: 1.17-6.26, P = 0.020), central venous cannulation (OR = 9.33, 95% CI: 3.06-28.43, P < 0.001), prolonged ICU stay (WMD = 10.37, 95% CI: 9.29-11.44, P < 0.001), methylprednisolone use (OR = 2.24, 95% CI: 1.24-4.04, P = 0.008), and the combination of methylprednisolone and Tocilizumab (OR = 4.54, 95% CI: 1.09-18.88, P = 0.037) were risk factors for ICU-BSI in COVID-19 patients.
Conclusion: We identified 10 risk factors for ICU-BSI in COVID-19 patients. In future studies, these factors can be combined to establish a more comprehensive and accurate prediction model for ICU-BSI in COVID-19 patients. Targeted measures can be taken earlier to control BSI.
Keywords: Bloodstream infection; COVID-19; ICU; Meta-analysis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Adrie C, Garrouste-Orgeas M, Ibn Essaied W, Schwebel C, Darmon M, Mourvillier B, Ruckly S, Dumenil AS, Kallel H, Argaud L, et al. Attributable mortality of ICU-acquired bloodstream infections: impact of the source, causative micro-organism, resistance profile and antimicrobial therapy. J Infect. 2017;74(2):131–41. - DOI - PubMed
-
- Llitjos J-F, Bredin S, Lascarrou J-B, Soumagne T, Cojocaru M, Leclerc M, Lepetit A, Gouhier A, Charpentier J, Piton G, et al. Increased susceptibility to intensive care unit-acquired pneumonia in severe COVID-19 patients: a multicentre retrospective cohort study. Ann Intensive Care. 2021;11(1):20. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
