

Enhanced myocardial perfusion in late gestation fetal lambs with impaired left ventricular inflow
- PMID: 39754538
- PMCID: PMC12579524
- DOI: 10.1113/JP286685
Enhanced myocardial perfusion in late gestation fetal lambs with impaired left ventricular inflow
Abstract
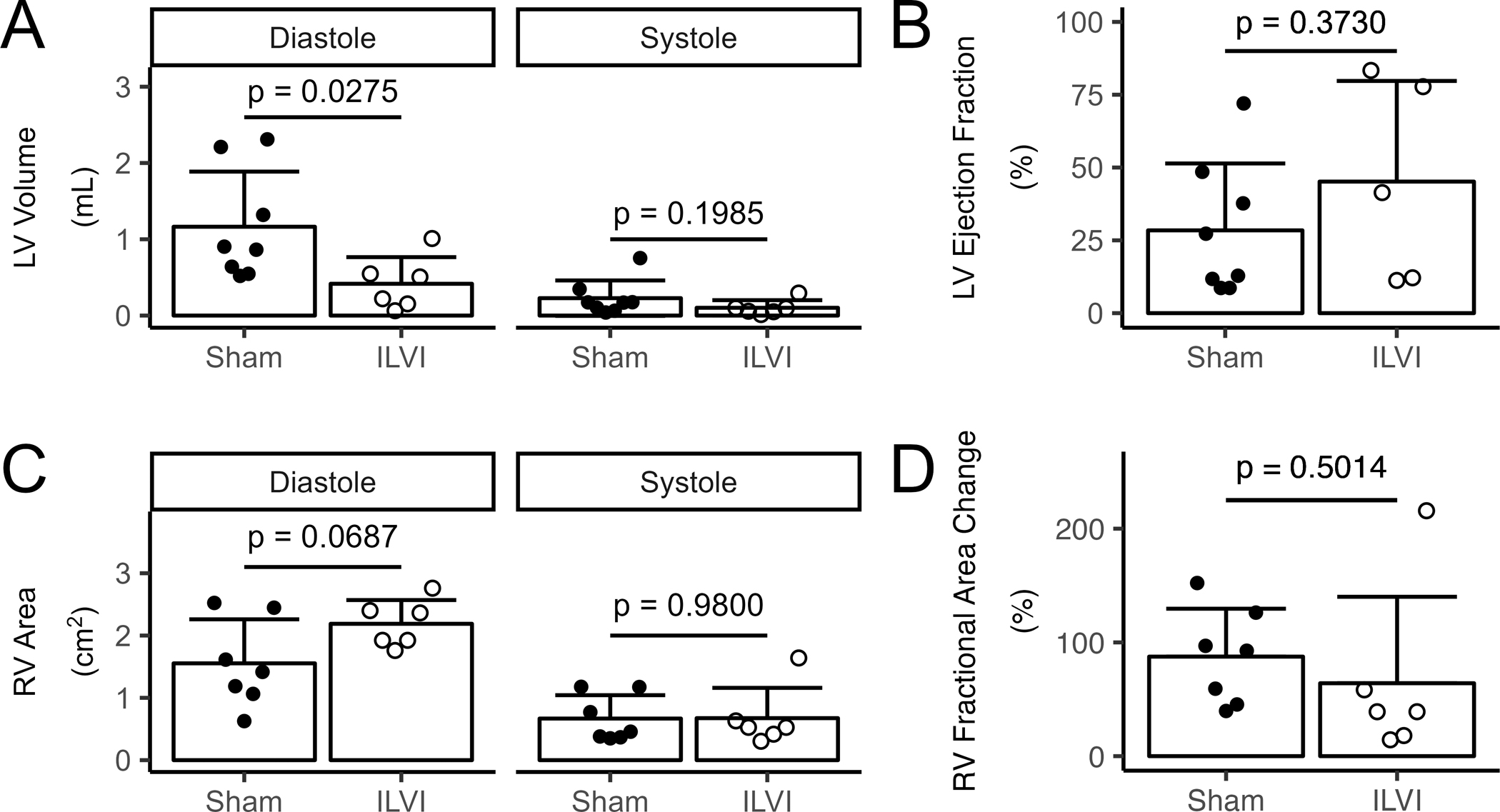
Robust preclinical models of asymmetric ventricular loading in late gestation reflecting conditions such as hypoplastic left heart syndrome are lacking. We characterized the morphometry and microvascular function of the hypoplastic left ventricle (LV) and remaining right ventricle (RV) in a sham-controlled late gestation fetal lamb model of impaired left ventricular inflow (ILVI). Singleton fetuses were instrumented at ∼120 days gestational age (dGA; term is ∼147 days) with vascular catheters, an aortic flow probe and a deflated left atrial balloon. Balloons in ILVI fetuses were inflated over the 8 day study until aortic output was eliminated; Sham balloons remained deflated. At the study end-point (∼134 dGA), cardiac function was assessed by echocardiography, microvascular perfusion of each free wall was measured by myocardial contrast echocardiography (MCE) and terminal morphometric data were collected. During the chronic study, flow through the ascending aorta of ILVI fetuses fell from 389 to -48 mL min-1 with minimal changes to other haemodynamics or blood chemistry. End-point echocardiography and morphometry similarly showed significant and meaningful reductions in ILVI LV chamber volume and wall mass without statistically significant changes in RV size relative to Shams. MCE revealed modestly increased LV perfusion and profoundly increased RV perfusion in ILVI fetuses. Our model displays effective LV hypoplasia with preserved overall fetal health, and our finding of increased RV myocardial perfusion may indicate active vascular remodelling in response to the experimental lesion. KEY POINTS: Hypoplastic left heart syndrome can be caused by insufficient inflow of blood to the fetal left ventricle. We found that eliminating fetal left ventricular input for 8 days reduced left ventricular size and volume, with minimal effects on the right ventricle or overall fetal health. Blood and oxygen delivery increased significantly in the right ventricle and slightly in the hypoplastic left ventricle. Our results suggest functional and anatomical adaptation of the fetal coronary microvasculature to univentricular right heart conditions.
Keywords: coronary microvascular function; development; fetus; heart; hypoplastic left heart; vascular remodelling.
© 2025 The Authors. The Journal of Physiology © 2025 The Physiological Society.
Conflict of interest statement
The authors declare no competing interests.
Figures





References
-
- Alanne L, Bhide A, Lantto J, Huhta H, Kokki M, Haapsamo M, Acharya G & Räsänen J (2021). Nifedipine disturbs fetal cardiac function during hypoxemia in a chronic sheep model at near term gestation. American Journal of Obstetrics and Gynecology 225, 544.e1–544.e9. - PubMed
-
- Bader D, Kugelman A, Lanir A, Tamir A, Mula E & Riskin A (2006). Cardiac troponin I serum concentrations in newborns: A study and review of the literature. Clinica Chimica Acta 371, 61–65. - PubMed
-
- Barbera A, Giraud GD, Reller MD, Maylie J, Morton MJ & Thornburg KL (2000). Right ventricular systolic pressure load alters myocyte maturation in fetal sheep. Am J Physiol Regul Integr Comp Physiol 279, R1157–1164. - PubMed
-
- Broberg CS, Giraud GD, Schultz JM, Thornburg KL, Hohimer AR & Davis LE (2003). Fetal anemia leads to augmented contractile response to hypoxic stress in adulthood. Am J Physiol Regul Integr Comp Physiol 285, R649–655. - PubMed
-
- Brooks PA, Khoo NS, Mackie AS & Hornberger LK (2012). Right Ventricular Function in Fetal Hypoplastic Left Heart Syndrome. Journal of the American Society of Echocardiography 25, 1068–1074. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous