

Results of a patient-level pooled analysis of three studies of trastuzumab deruxtecan in HER2-positive breast cancer with active brain metastasis
- PMID: 39754978
- PMCID: PMC11758132
- DOI: 10.1016/j.esmoop.2024.104092
Results of a patient-level pooled analysis of three studies of trastuzumab deruxtecan in HER2-positive breast cancer with active brain metastasis
Abstract
Background: Brain metastases (BMs) are common in human epidermal growth factor receptor 2 (HER2)-positive advanced breast cancer, increasing morbidity and mortality. Systemic therapy for BMs can be effective, with the triple combination of trastuzumab, capecitabine, and tucatinib being a potential standard. More recently, intracranial activity of antibody-drug conjugates has been reported, but the size of individual studies has been small. Therefore, this patient-level pooled analysis was conducted.
Patients and methods: This is a patient-level pooled analysis of the prospective phase II DEBBRAH and TUXEDO-1 trials and the retrospective DFCI/Duke/MDACC cohort. Patients with evaluable active BMs (defined as newly diagnosed and untreated or progressing with measurable tumor-related size after previous local therapy) from HER2-positive breast cancer (BC) and treated with trastuzumab deruxtecan (T-DXd) included in these studies were eligible. The primary endpoint was intracranial objective response rate (ORR-IC) by Response Assessment in Neuro-Oncology (RANO)-BM criteria.
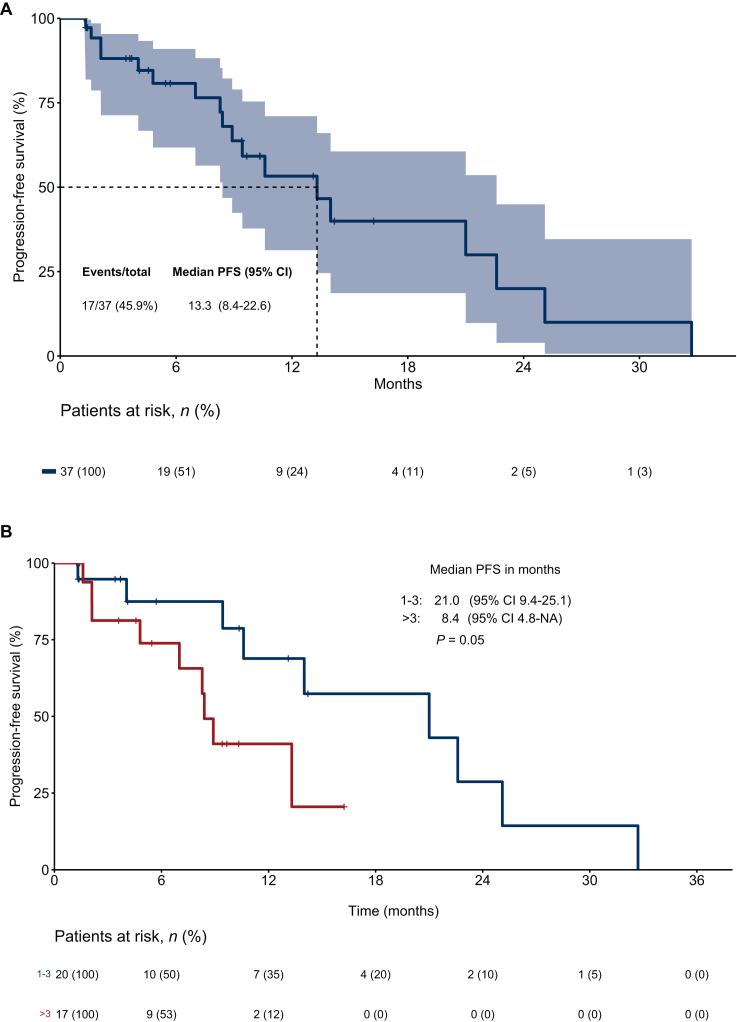
Results: Overall, 37 patients were assessable for intracranial response assessment. BMs progressing after prior local therapy were present in 64.9% of patients. The median patient age was 49.1 years. All patients had received prior trastuzumab and the median number of prior systemic treatment lines was 3 (0-13). The pooled ORR-IC by RANO-BM criteria was 64.9% [95% confidence interval (CI) 47.5% to 79.8%] with low heterogeneity observed between the studies included. The clinical benefit rate by RANO-BM was 81.1% (95% CI 64.8% to 92.0%). The median progression-free survival was 13.3 months (95% CI 8.4-22.6 months) and the median overall survival was 22.5 months (95% CI 14.9 months-not achieved) with high heterogeneity between studies and numerically longer in patients with few prior treatment lines. Quality of life remained stable throughout treatment, with no new safety concerns.
Conclusions: This patient-level pooled analysis of DEBBRAH, TUXEDO-1, and the DFCI/Duke/MDACC cohort indicates clinically relevant intracranial activity of T-DXd in patients with active HER2-positive BC, BMs, and extensive systemic pretreatment. The results therefore support the use of T-DXd when clinically indicated irrespective of BMs.
Keywords: HER2-positive breast cancer; active brain metastases; systemic therapy; trastuzumab deruxtecan.
Copyright © 2024 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures



References
-
- Witzel I., Laakmann E., Weide R., et al. Treatment and outcomes of patients in the brain metastases in breast cancer network registry. Eur J Cancer. 2018;102:1–9. - PubMed
-
- Heitz F., Harter P., Lueck H.J., et al. Triple-negative and HER2-overexpressing breast cancers exhibit an elevated risk and an earlier occurrence of cerebral metastases. Eur J Cancer. 2009;45:2792–2798. - PubMed
-
- Lin N.U., Winer E.P. Brain metastases: the HER2 paradigm. Clin Cancer Res. 2007;13:1648–1655. - PubMed
-
- Mamounas E.P., Untch M., Mano M.S., et al. Adjuvant T-DM1 versus trastuzumab in patients with residual invasive disease after neoadjuvant therapy for HER2-positive breast cancer: subgroup analyses from KATHERINE. Ann Oncol. 2021;32:1005–1014. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
