

Economic impact of prolonged tracheal extubation times on operating room time overall and for subgroups of surgeons: a historical cohort study
- PMID: 39755614
- PMCID: PMC11699662
- DOI: 10.1186/s12871-024-02862-6
Economic impact of prolonged tracheal extubation times on operating room time overall and for subgroups of surgeons: a historical cohort study
Abstract
Background: Prolonged tracheal extubation time is defined as an interval ≥ 15 min from the end of surgery to extubation. An earlier study showed that prolonged extubations had a mean 12.4 min longer time from the end of surgery to operating room (OR) exit. Prolonged extubations usually (57%) were observed during OR days with > 8 h of cases and turnovers, such that longer OR times from prolonged extubation can be treated as a variable cost (i.e., each added minute incurs an expense). The current study addressed limitations of the generalizability of these earlier investigations.
Methods: The retrospective cohort study included cases performed at a university hospital October 2011 through June 2023 with general anesthesia, tracheal intubation and extubation in the OR where the anesthetic was performed, and non-prone positioning. The primary endpoint was the interval from end of surgery to OR exit. Mean OR time differences with/without prolonged extubation were analyzed pairwise by surgeon. The variance among surgeons was estimated using the DerSimonian-Laird method with Knapp-Hartung adjustment for the sample sizes of surgeons. Proportions were analyzed after arcsine transformation, and the inverse taken to report results.
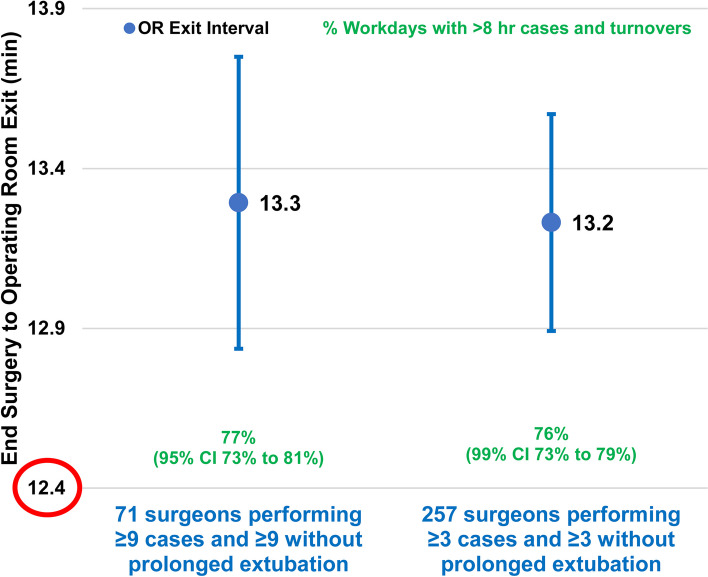
Results: There were prolonged extubations for 23% (41,768/182,374) of cases. Prolonged extubations had a mean 13.3 min longer time from the end of surgery to OR exit (95% confidence interval 12.8-13.7 min, P < 0.0001). That result was among the 71 surgeons each with ≥ 9 cases having prolonged extubation times and ≥ 9 cases with typical extubation times. Results were similar using a threshold of ≥ 3 cases, comprising 257 surgeons (13.2 min, P < 0.0001). Among the 71 surgeons with at least nine prolonged extubations, on most days with a prolonged extubation during at least one of their cases, there were > 8 h of cases and turnover times in the OR (77%, 73%-81%, P < 0.0001). Results were similar when analyzed for the 249 surgeons each with ≥ 3 cases with prolonged extubation (76%, P < 0.0001).
Conclusions: Matching earlier findings, prolonged tracheal extubation times are important economically, increasing OR time by 13 min and usually performed in ORs with lists of cases of sufficient duration to treat the extra time as a variable cost.
Keywords: Airway extubation; Anesthetics; Inhalational; Models; Operating rooms; Statistical.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The University of Iowa Institutional Review Board determined that this retrospective cohort study #202306541 does not meet the regulatory definition of human subjects research. The University of Iowa IRB therefore deemed that additional ethical approval and informed consent were unnecessary according to US national regulations. The IRB determination letter is included in supplemental content. There is no clinical trial number because this is not a clinical trial. A tutorial on US law prepared by the US Office for Human Research Protections that describes what is not human subjects research starts on page 8: https://www.hhs.gov/ohrp/sites/default/files/OHRP-HHS-Learning-Module-Lesson2.pdf#page=8 . Consent for publication: Not applicable. Competing interests: The Division of Management Consulting of the University of Iowa’s Department of Anesthesia provides consultations to hospitals and corporations. Dr. Dexter receives no funds personally other than his salary and allowable expense reimbursements from the University of Iowa and has tenure with no incentive program. He and his family have no financial holdings in any company related to his work other than indirectly through mutual funds for retirement. Income from the Division's consulting work is used to fund Division research. A list of all the Division’s consults is available in his posted curriculum vitae at https://FranklinDexter.net/Contact_Info.htm . Drs. Marian and Epstein have no competing interests. The opinions expressed in this paper are those of the authors and do not necessarily represent those of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA.
Figures
Similar articles
-
Increased mean time from end of surgery to operating room exit in a historical cohort of cases with prolonged time to extubation.Anesth Analg. 2013 Dec;117(6):1453-9. doi: 10.1213/ANE.0b013e3182a44d86. Anesth Analg. 2013. PMID: 24257395
-
Narrative Review of Prolonged Times to Tracheal Extubation After General Anesthesia With Intubation and Extubation in the Operating Room.Anesth Analg. 2024 Apr 1;138(4):775-781. doi: 10.1213/ANE.0000000000006644. Epub 2023 Oct 3. Anesth Analg. 2024. PMID: 37788413 Review.
-
Cohort study of cases with prolonged tracheal extubation times to examine the relationship with duration of workday.Can J Anaesth. 2013 Nov;60(11):1070-6. doi: 10.1007/s12630-013-0025-5. Epub 2013 Sep 14. Can J Anaesth. 2013. PMID: 24037748
-
Comparison of Percentage Prolonged Times to Tracheal Extubation Between a Japanese Teaching Hospital and One in the United States, Without and With a Phase I Postanesthesia Care Unit.Anesth Analg. 2021 Nov 1;133(5):1206-1214. doi: 10.1213/ANE.0000000000005231. Anesth Analg. 2021. PMID: 33044261
-
Exceedance Probabilities of Log-normal Distributions for One Group, Two Groups, and Meta-analysis of Multiple Two-group Studies, With Application to Analyses of Prolonged Times to Tracheal Extubation.J Med Syst. 2023 Apr 19;47(1):49. doi: 10.1007/s10916-023-01935-2. J Med Syst. 2023. PMID: 37074507 Review.
References
-
- Dexter F, Bayman EO, Epstein RH. Statistical modeling of average and variability of time to extubation for meta-analysis comparing desflurane to sevoflurane. Anesth Analg. 2010;110:570–80. 10.1213/ANE.0b013e3181b5dcb7. - PubMed
-
- Dexter F, Epstein RH. Increased mean time from end of surgery to operating room exit in a historical cohort of cases with prolonged time to extubation. Anesth Analg. 2013;117:1453–9. 10.1213/ANE.0b013e3182a44d86. - PubMed
-
- Epstein RH, Dexter F, Brull SJ. Cohort study of cases with prolonged tracheal extubation times to study relationship with durations of workdays. Can J Anesth. 2013;60:1070–6. 10.1007/s12630-013-0025-5. - PubMed
-
- Dexter F, Epstein RH. Typical savings from each minute reduction in tardy first case of the day starts. Anesth Analg. 2009;108:1262–7. 10.1213/ane.0b013e31819775cd. - PubMed
-
- Dexter F, Epstein RH, Penning DH. Late first-case of the day starts do not cause greater minutes of over-utilized time at an endoscopy suite with 8-hour workdays and late running rooms. A historical cohort study. J Clin Anesth. 2020; 59:18–25. 10.1016/j.jclinane.2019.06.013. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
