

Antithrombin III deficiency and idiopathic intracranial hypertension: a case report
- PMID: 39755655
- PMCID: PMC11700454
- DOI: 10.1186/s13256-024-04997-z
Antithrombin III deficiency and idiopathic intracranial hypertension: a case report
Abstract
Background: Idiopathic intracranial hypertension (IIH) is a condition where the pressure of the cerebrospinal fluid in the brain increases without a known cause. It typically affects adults but can also occur in adolescents and children, although it is less common. Numerous elements, including coagulopathy, have been documented in previous cases as potential etiological factors of IIH. Nonetheless, our objective was to present the insufficiency of a coagulation factor as an additional contributing factor to IIH, a notion that has not been previously reported.
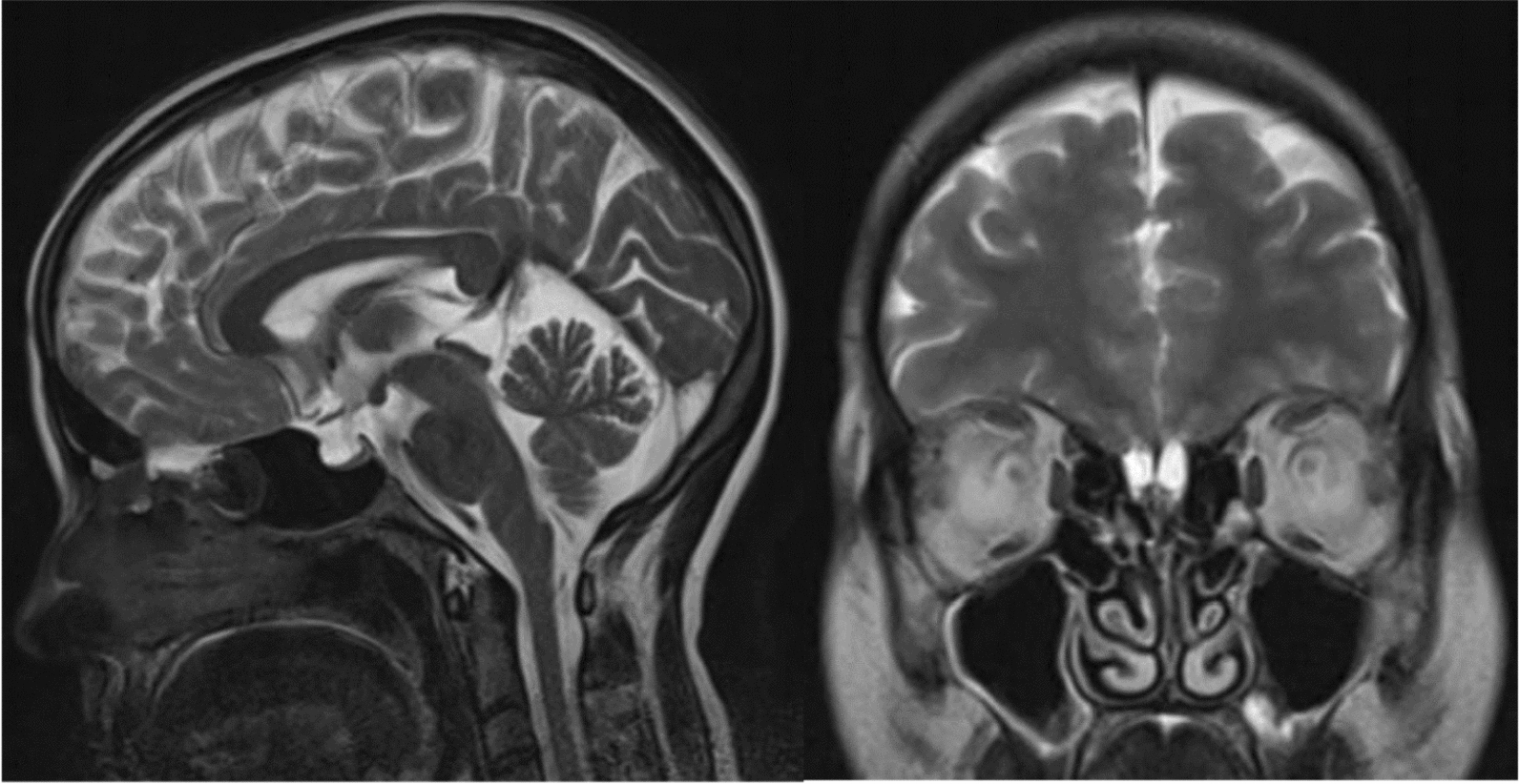
Case presentation: In this case, a 34-year-old West Asian female patient presented with a subacute generalized headache, bilateral blurred vision, and papilledema. The patient's brain magnetic resonance imaging showed flattening of the posterior globe and empty sella, but no other abnormalities were detected. The results of magnetic resonance venography and cerebrospinal fluid analysis were also normal, except for an opening cerebrospinal fluid pressure of 600 mm H2O during the lumbar puncture. Rheumatologic and endocrine disorders were ruled out on the basis of clinical assessment and laboratory tests. The patient was started on acetazolamide (1 g/day, increased to 2 g/day) and furosemide (20 mg/twice a day) and was encouraged to lose weight. These treatments led to some improvement for about 1 year, but her symptoms then worsened without an obvious cause. Given the prolonged duration of the disease and the lack of expected response to treatment, the patient was reevaluated for endocrinopathy and collagen vascular disease, which were negative. An additional workup revealed an antithrombin III (AT III) deficiency, for which the patient was prescribed acetylsalicylic acid (80 mg/day) in addition to the previous medications. As a result, the patient's papilledema, macular thickness, and nerve fiber layer edema decreased, as observed by fundoscopy and optical coherence tomography. Clinical examination and imaging also showed improvement in the patient's symptoms.
Conclusion: This case highlights the importance of considering coagulopathy in cases of IIH and suggests that antiplatelet therapy with acetylsalicylic acid may be beneficial for such patients.
Keywords: Antithrombin III deficiency; Headache; Idiopathic intracranial hypertension; Papilledema; Pseudotumor cerebri.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by Tehran University of Medical Sciences. The details of this study were explained to the patient, and the patient provided informed consent to participate in the project. Consent for publication: Written informed consent was obtained from the patient for publication of this study and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Can Lumbar Puncture Be Safely Deferred in Patients With Mild Presumed Idiopathic Intracranial Hypertension?J Neuroophthalmol. 2022 Dec 1;42(4):505-508. doi: 10.1097/WNO.0000000000001411. Epub 2021 Oct 22. J Neuroophthalmol. 2022. PMID: 34860748
-
Idiopathic intracranial hypertension presenting with isolated unilateral facial nerve palsy: a case report.J Med Case Rep. 2019 Apr 19;13(1):94. doi: 10.1186/s13256-019-2060-5. J Med Case Rep. 2019. PMID: 30999940 Free PMC article.
-
Update on Idiopathic Intracranial Hypertension.Neurol Clin. 2017 Feb;35(1):45-57. doi: 10.1016/j.ncl.2016.08.004. Neurol Clin. 2017. PMID: 27886895 Free PMC article. Review.
-
External lumbar drainage in progressive pediatric idiopathic intracranial hypertension.J Neurosurg Pediatr. 2021 Jul 16;28(4):490-496. doi: 10.3171/2021.2.PEDS2143. Print 2021 Oct 1. J Neurosurg Pediatr. 2021. PMID: 34271543
-
Diagnosis and treatment of idiopathic intracranial hypertension.Cephalalgia. 2021 Apr;41(4):472-478. doi: 10.1177/0333102421997093. Epub 2021 Feb 25. Cephalalgia. 2021. PMID: 33631966 Free PMC article. Review.
References
-
- Markey KA, Mollan SP, Jensen RH, Sinclair AJ. Understanding idiopathic intracranial hypertension: mechanisms, management, and future directions. Lancet Neurol. 2016;15(1):78–91. - PubMed
-
- Friedman DI, Jacobson DM. Diagnostic criteria for idiopathic intracranial hypertension. Neurology. 2002;59(10):1492–5. - PubMed
-
- Robelin F, Lenfant M, Ricolfi F, Béjot Y, Comby PO. Idiopathic intracranial hypertension: from physiopathological mechanisms to therapeutic decision. Rev Med Interne. 2022;43(11):661–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
