

Advancing a machine learning-based decision support tool for pre-hospital assessment of dyspnoea by emergency medical service clinicians: a retrospective observational study
- PMID: 39757181
- PMCID: PMC11702062
- DOI: 10.1186/s12873-024-01166-9
Advancing a machine learning-based decision support tool for pre-hospital assessment of dyspnoea by emergency medical service clinicians: a retrospective observational study
Abstract
Background: In Sweden with about 10 million inhabitants, there are about one million primary ambulance missions every year. Among them, around 10% are assessed by Emergency Medical Service (EMS) clinicians with the primary symptom of dyspnoea. The risk of death among these patients has been reported to be remarkably high, at 11,1% and 13,2%. The aim was to develop a Machine Learning (ML) model to provide support in assessing patients in pre-hospital settings and to compare them with established triage tools.
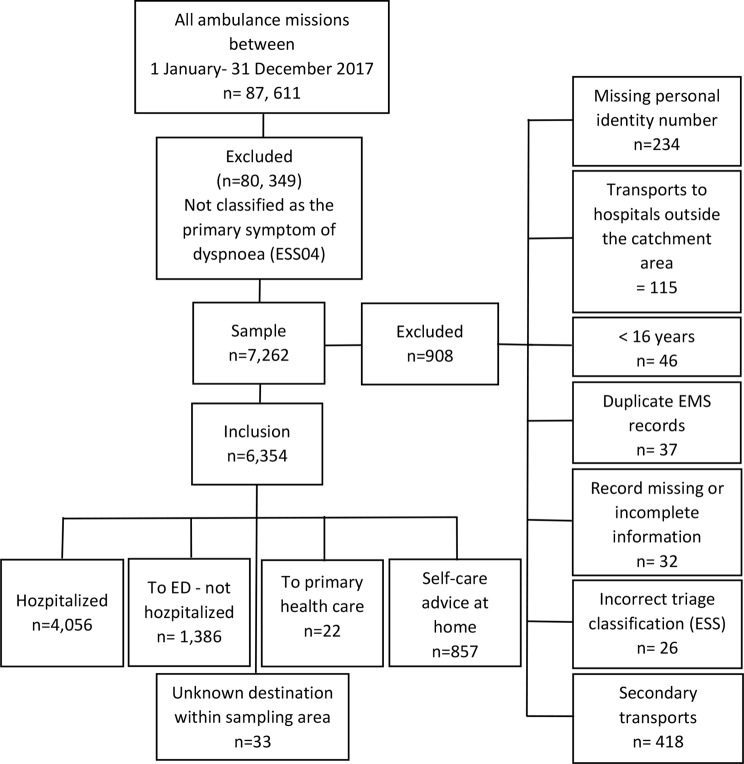
Methods: This was a retrospective observational study including 6,354 patients who called the Swedish emergency telephone number (112) between January and December 2017. Patients presenting with the main symptom of dyspnoea were included which were recruited from two EMS organisations in Göteborg and Södra Älvsborg. Serious Adverse Event (SAE) was used as outcome, defined as any of the following:1) death within 30 days after call for an ambulance, 2) a final diagnosis defined as time-sensitive, 3) admitted to intensive care unit, or 4) readmission within 72 h and admitted to hospital receiving a final time-sensitive diagnosis. Logistic regression, LASSO logistic regression and gradient boosting were compared to the Rapid Emergency Triage and Treatment System for Adults (RETTS-A) and National Early Warning Score2 (NEWS2) with respect to discrimination and calibration of predictions. Eighty percent (80%) of the data was used for model development and 20% for model validation.
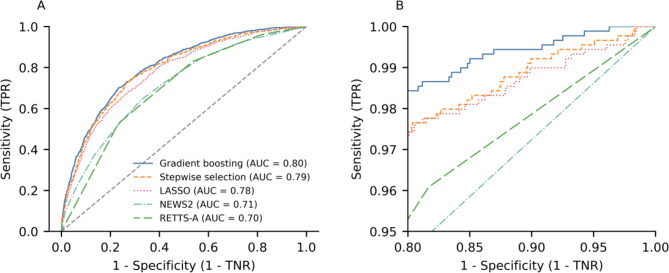
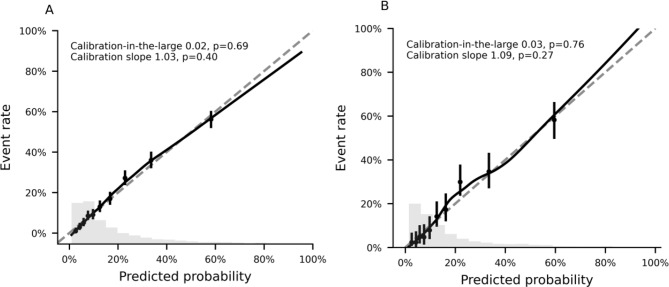
Results: All ML models showed better performance than RETTS-A and NEWS2 with respect to all evaluated performance metrics. The gradient boosting algorithm had the overall best performance, with excellent calibration of the predictions, and consistently showed higher sensitivity to detect SAE than the other methods. The ROC AUC on test data increased from 0.73 (95% CI 0.70-0.76) with RETTS-A to 0.81 (95% CI 0.78-0.84) using gradient boosting.
Conclusions: Among 6,354 ambulance missions caused by patients suffering from dyspnoea, an ML method using gradient boosting demonstrated excellent performance for predicting SAE, with substantial improvement over the more established methods RETTS-A and NEWS2.
Keywords: Ambulance; Decision support tool; Dyspnoea; Emergency medical services; Machine learning; Prehospital; Serious adverse event.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study received approval from The Regional Ethical Review Board in Gothenburg, Sweden (Dnr 989–17) and adhered to the ethical standards of the Declaration of Helsinki [46]. Consent for data analysis was obtained from the chief executive officers of the two EMS organisations. In accordance with Swedish law, informed consent was not required for participation due to the disproportionate work effort involved. Also, some patients, couldn’t provide retrospective informed consent due to poor health or death, minimizing the risk of selection bias. Patient confidentiality was upheld by translating identification numbers into unique codes. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Pre-hospital predictors of an adverse outcome among patients with dyspnoea as the main symptom assessed by pre-hospital emergency nurses - a retrospective observational study.BMC Emerg Med. 2020 Nov 10;20(1):89. doi: 10.1186/s12873-020-00384-1. BMC Emerg Med. 2020. PMID: 33172409 Free PMC article.
-
Pre-hospital triage performance and emergency medical services nurse's field assessment in an unselected patient population attended to by the emergency medical services: a prospective observational study.Scand J Trauma Resusc Emerg Med. 2020 Aug 17;28(1):81. doi: 10.1186/s13049-020-00766-1. Scand J Trauma Resusc Emerg Med. 2020. PMID: 32807224 Free PMC article.
-
A validation of machine learning-based risk scores in the prehospital setting.PLoS One. 2019 Dec 13;14(12):e0226518. doi: 10.1371/journal.pone.0226518. eCollection 2019. PLoS One. 2019. PMID: 31834920 Free PMC article.
-
A Machine Learning Approach to Predicting Need for Hospitalization for Pediatric Asthma Exacerbation at the Time of Emergency Department Triage.Acad Emerg Med. 2018 Dec;25(12):1463-1470. doi: 10.1111/acem.13655. Epub 2018 Nov 29. Acad Emerg Med. 2018. PMID: 30382605
-
Applications and Performance of Machine Learning Algorithms in Emergency Medical Services: A Scoping Review.Prehosp Disaster Med. 2024 Oct;39(5):368-378. doi: 10.1017/S1049023X24000414. Epub 2024 May 17. Prehosp Disaster Med. 2024. PMID: 38757150 Free PMC article.
Cited by
-
Mapping artificial intelligence models in emergency medicine: A scoping review on artificial intelligence performance in emergency care and education.Turk J Emerg Med. 2025 Apr 1;25(2):67-91. doi: 10.4103/tjem.tjem_45_25. eCollection 2025 Apr-Jun. Turk J Emerg Med. 2025. PMID: 40248473 Free PMC article. Review.
References
-
- Herlitz J, Magnusson C, Andersson Hagiwara M, Lundgren P, Larsson G, Rawshani A, Axelsson C. Den prehospitala akutsjukvården i Sverige har stora utmaningar [Eng:The pre-hospital emergency care in Sweden faces significant challenges]. Läkartidningen. 2021;118:21119. Available from: https://lakartidningen.se/wp-content/uploads/2021/10/21119.pdf. Accessed 4 aug 2024. - PubMed
-
- Beygui F, Castren M, Brunetti ND, Rosell-Ortiz F, Christ M, Zeymer U, et al. Pre-hospital management of patients with chest pain and/or dyspnoea of cardiac origin. A position paper of the Acute Cardiovascular Care Association (ACCA) of the ESC. Eur Heart J Acute Cardiovasc Care. 2020;9(1suppl):59–81. 10.1177/2048872615604119. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
