

An atypical presentation of Wernicke-Korsakoff encephalopathy mimicking a left hemispheric stroke: case report
- PMID: 39758439
- PMCID: PMC11696281
- DOI: 10.3389/fpsyt.2024.1499803
An atypical presentation of Wernicke-Korsakoff encephalopathy mimicking a left hemispheric stroke: case report
Abstract
Background: Wernicke-Korsakoff encephalopathy is a metabolic disease caused by vitamin B1 deficiency that predominantly affects alcoholic patients. Its clinical picture is characterized mainly by altered mental status with memory deficits, ophthalmoparesis, and ataxia, although other clinical manifestations may also be present. The current case presents certain clinical difficulties regarding the diagnosis when confronting an atypical presentation of a classical disease in an acute setting when a decision to administer an intravenous thrombolytic agent needs to be made.
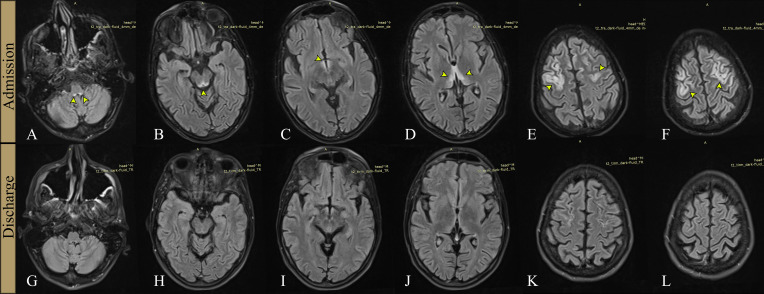
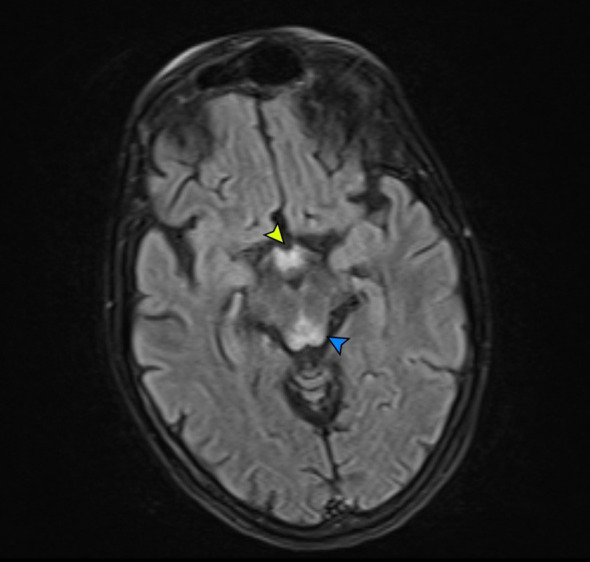
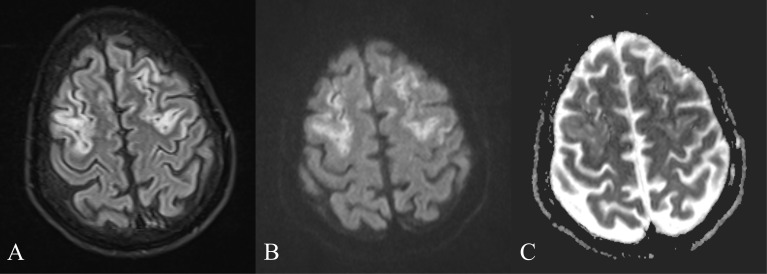
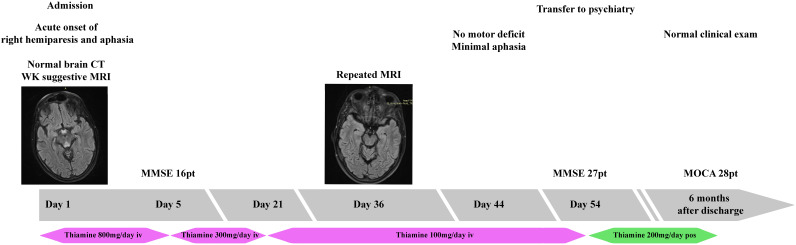
Case presentation: This case involves a young male patient, with a history of chronic alcohol abuse, malnourished, and in poor general health, who presented with right-sided hemiparesis and language disturbance of acute onset, suggesting a left hemispheric stroke. The psychological examination was difficult due to a mix of confusion and aphasia, the latter being challenging to assess as the patient had a dismissive and highly deflective attitude toward the examiner. The initial cerebral computed tomography scan was unremarkable, in line with early imaging in ischemic stroke patients. On subsequent magnetic resonance imaging, lesions were observed in the medullo-pontine tegmentum, around the aqueduct of Sylvius, in the mamillary bodies, in the medial thalami, but also extensive bilateral cortical involvement in the frontal lobes. After receiving intravenous vitamin B1 treatment, the patient made a slow, but full, recovery, after eight weeks of hospitalization, and was subsequently transferred to a psychiatry clinic for treatment of his addiction.
Conclusion: Atypical Wernicke-Korsakoff encephalopathy can closely mimic stroke, usually akin to a vertebro-basilar lesion. Our case is the first report we are aware of Wernicke-Korsakoff encephalopathy feigning a left hemispheric stroke with aphasia and right hemiparesis. This has implications for the emergency medicine doctor, neurologist and the stroke specialist when considering an emergency differential diagnosis for a patient with an initial normal computed tomography scan, especially in regard to deciding acute therapy.
Keywords: Wernicke-Korsakoff; case report; encephalopathy; stroke mimic; thiamine.
Copyright © 2024 Butnariu, Anghel, Ciobanu, Cojocaru, Antonescu-Ghelmez, Manea and Antonescu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A Clinician's View of Wernicke-Korsakoff Syndrome.J Clin Med. 2022 Nov 15;11(22):6755. doi: 10.3390/jcm11226755. J Clin Med. 2022. PMID: 36431232 Free PMC article. Review.
-
Need for early diagnosis of mental and mobility changes in Wernicke encephalopathy.Cogn Behav Neurol. 2014 Dec;27(4):215-21. doi: 10.1097/WNN.0000000000000041. Cogn Behav Neurol. 2014. PMID: 25539041
-
Fetal demise and Wernicke-Korsakoff syndrome in a patient with hyperemesis gravidarum: a case report.J Med Case Rep. 2023 Feb 2;17(1):32. doi: 10.1186/s13256-022-03748-2. J Med Case Rep. 2023. PMID: 36726136 Free PMC article.
-
Wernicke Encephalopathy in an Elderly Patient Due to Chronic Malnutrition From an Atypical Diet.Cureus. 2021 Mar 31;13(3):e14210. doi: 10.7759/cureus.14210. Cureus. 2021. PMID: 33948400 Free PMC article.
-
[Severe sepsis as an initial presentation in children with Wernicke' s encephalopathy: report of a case and literature review].Zhonghua Er Ke Za Zhi. 2011 Aug;49(8):612-6. Zhonghua Er Ke Za Zhi. 2011. PMID: 22093426 Review. Chinese.
References
Publication types
LinkOut - more resources
Full Text Sources