

Intracranial hemorrhage and additional anomalies detected on prenatal magnetic resonance imaging: A large, retrospective study in two tertiary medical institutions
- PMID: 39759338
- PMCID: PMC11696780
- DOI: 10.1016/j.heliyon.2024.e41037
Intracranial hemorrhage and additional anomalies detected on prenatal magnetic resonance imaging: A large, retrospective study in two tertiary medical institutions
Abstract
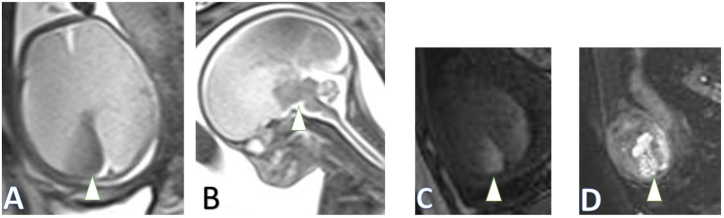
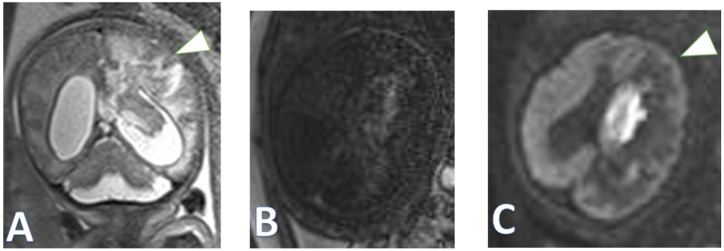
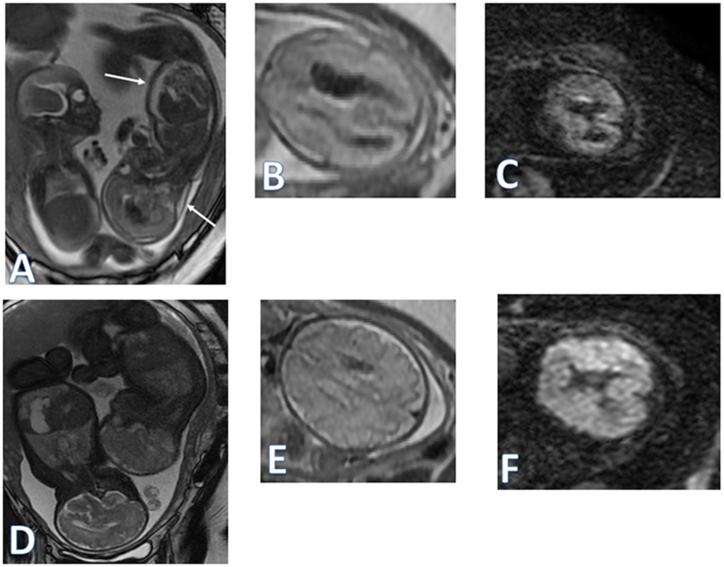
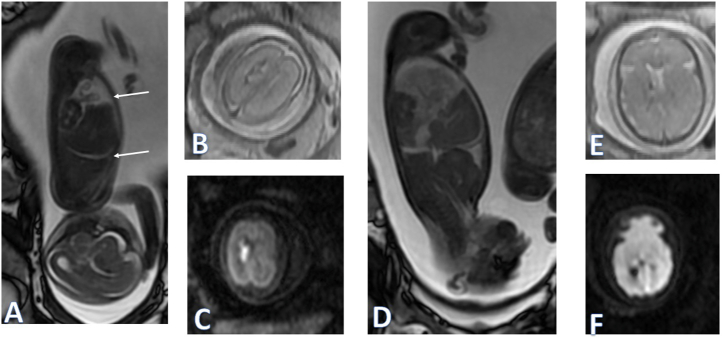
Objectives: To clarify the prenatal magnetic resonance (MR) imaging characteristics of fetal intracranial haemorrhages (ICHs) in a large cohort and correlate them with birth outcomes.
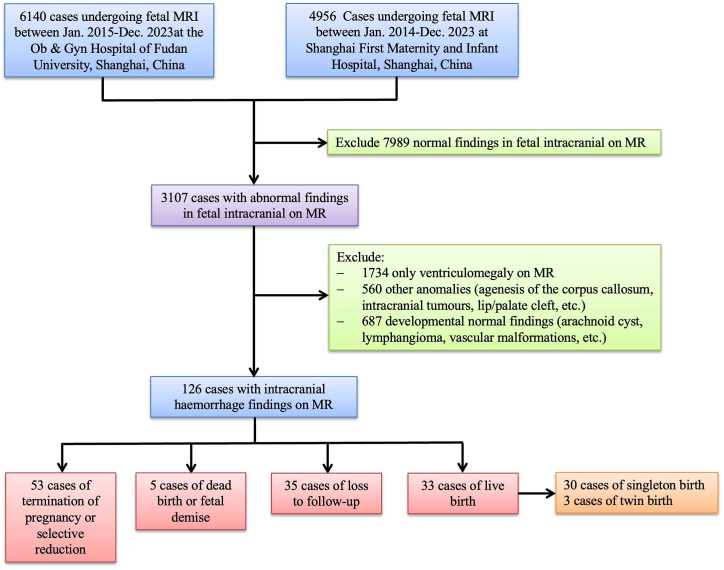
Methods: We retrospectively reviewed MR images of fetuses with ICH on screening ultrasound (US) on picture archiving communication system (PACS) servers within a nearly ten-year period from two medical tertiary centres. The indications, main abnormal findings and coexistent anomalies were recorded by two experienced radiologists with census readings.
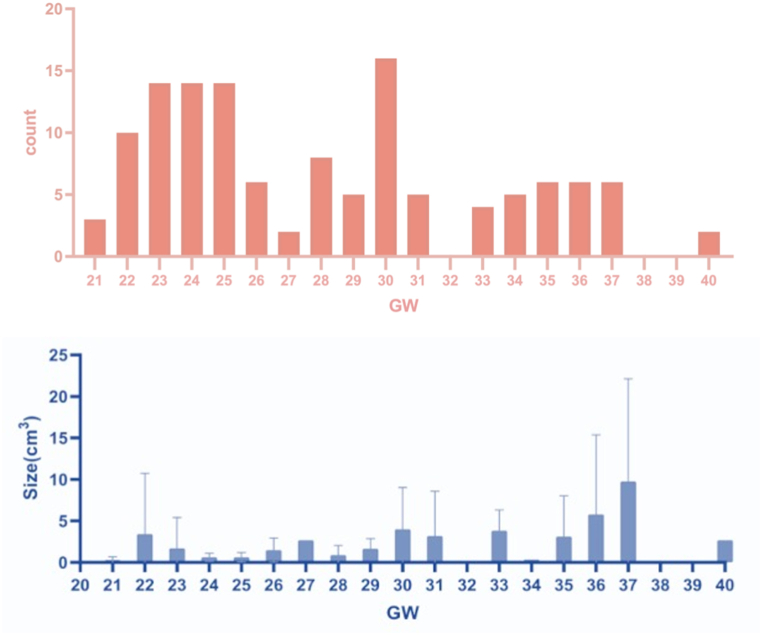
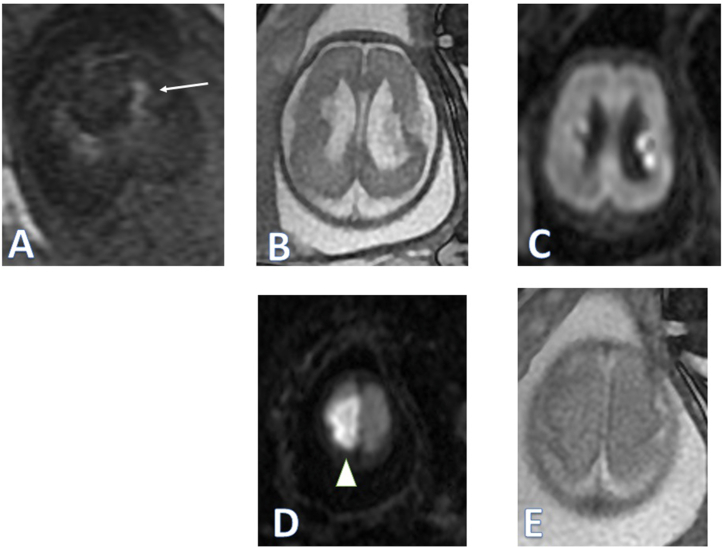
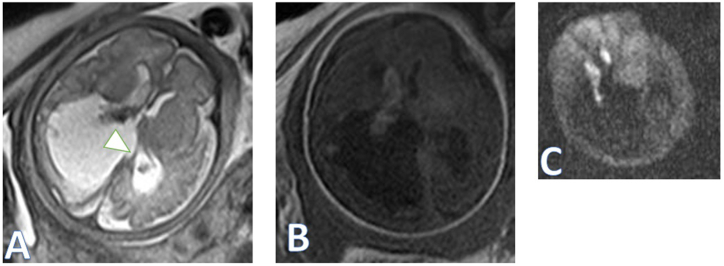
Results: We recruited 126 cases (average gestational week, 28.0 ± 5.0 weeks) with prenatal MR imaging, including 116 singleton pregnancies and 10 monochromic twin pregnancies. Predominant coexistent anomalies were ventriculomegaly (35.7 %), holoprosencephaly or porencephaly (13.4 %) and enlarged posterior fossa/or posterior fossa cyst (8.7 %) in the lesion-based evaluation. The number of haemorrhagic lesions and the occurrence of the detected complications did not show a correlation with the size of the haematoma. The mass effect of ICH was more commonly observed in the fetus with large for gestational age (GA) than that with small for GA.
Conclusions: Prenatal MR imaging could better show ICH morphology and associated abnormal findings. As a complementary tool of US, MR imaging could help with prenatal counselling and treatment selection after birth.
Keywords: Fetal malformation; Fetus; Intracranial hemorrhages; Magnetic resonance imaging.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Prenatal Magnetic Resonance Imaging helps Discover Cerebellar Dysplasia or Malformations in Foetuses.Curr Med Imaging. 2023 Oct 31. doi: 10.2174/0115734056256514231020103822. Online ahead of print. Curr Med Imaging. 2023. PMID: 37921151
-
Role of magnetic resonance imaging in fetuses with mild or moderate ventriculomegaly in the era of fetal neurosonography: systematic review and meta-analysis.Ultrasound Obstet Gynecol. 2019 Aug;54(2):164-171. doi: 10.1002/uog.20197. Epub 2019 Jul 11. Ultrasound Obstet Gynecol. 2019. PMID: 30549340
-
Role of prenatal magnetic resonance imaging in fetuses with isolated mild or moderate ventriculomegaly in the era of neurosonography: international multicenter study.Ultrasound Obstet Gynecol. 2020 Sep;56(3):340-347. doi: 10.1002/uog.21974. Ultrasound Obstet Gynecol. 2020. PMID: 31917496
-
Role of prenatal magnetic resonance imaging in fetuses with isolated severe ventriculomegaly at neurosonography: A multicenter study.Eur J Obstet Gynecol Reprod Biol. 2021 Dec;267:105-110. doi: 10.1016/j.ejogrb.2021.10.014. Epub 2021 Oct 23. Eur J Obstet Gynecol Reprod Biol. 2021. PMID: 34773875
-
Fetal MRI assessment of posterior fossa anomalies: A review.J Neuroimaging. 2021 Jul;31(4):620-640. doi: 10.1111/jon.12871. Epub 2021 May 8. J Neuroimaging. 2021. PMID: 33964092 Review.
References
-
- van der Knoop B.J., Zonnenberg I.A., Verbeke J.I.M.L., de Vries L.S., Pistorius L.R., van Weissenbruch M.M., et al. Additional value of advanced neurosonography and magnetic resonance imaging in fetuses at risk for brain damage. Ultrasound Obstet. Gynecol. 2020;56(3):348–358. doi: 10.1002/uog.21943. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
