

Herpes Simplex Pneumonitis Presenting As Acute Respiratory Distress Syndrome and Septic Shock
- PMID: 39759712
- PMCID: PMC11696180
- DOI: 10.7759/cureus.75075
Herpes Simplex Pneumonitis Presenting As Acute Respiratory Distress Syndrome and Septic Shock
Abstract
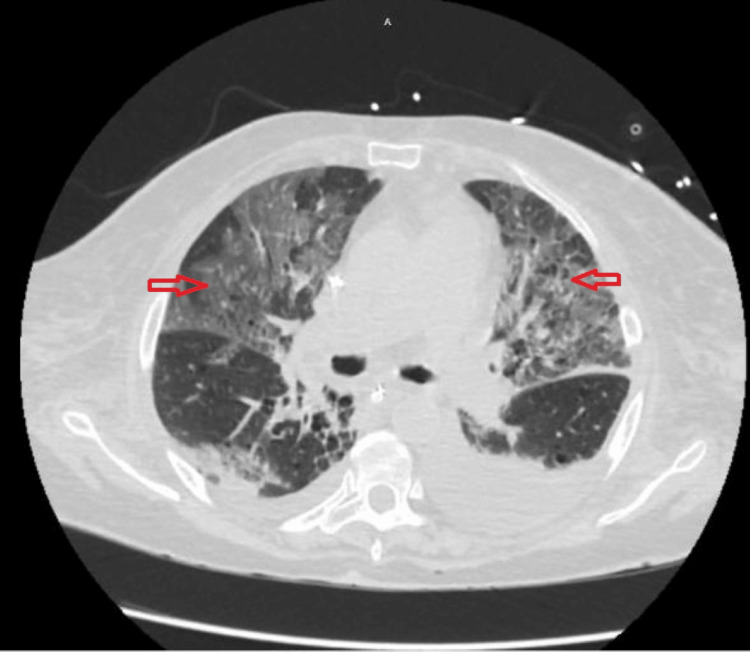
We present a case report of a 72-year-old female with a history of stage III rectal adenocarcinoma undergoing chemotherapy who developed neutropenic sepsis and acute respiratory failure. The patient was admitted to the intensive care unit (ICU) due to worsening respiratory status and was subsequently diagnosed with disseminated herpes simplex virus (HSV) infection including acute respiratory distress syndrome (ARDS). This case highlights the challenges in diagnosing and managing HSV infection in critically ill patients and emphasizes the importance of early recognition and appropriate treatment in improving patient outcomes. This case underscores the significance of considering viral etiologies, such as HSV, in patients with unexplained respiratory symptoms presenting as ARDS.
Keywords: acute respiratory distress syndrome (ards); acute respiratory failure; disseminated herpes simplex virus infection; herpes simplex virus; herpetic tracheobronchitis; hsv pneumonia; immunocompromised patients; neutropenic sepsis; septic shock; septic shock (ss).
Copyright © 2024, Pata et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures



References
-
- Herpes simplex virus type 1 and respiratory disease in critically-ill patients: real pathogen or innocent bystander? Simoons-Smit AM, Kraan EM, Beishuizen A, Strack van Schijndel RJ, Vandenbroucke-Grauls CM. Clin Microbiol Infect. 2006;12:1050–1059. - PubMed
-
- Herpes simplex virus lung infection in patients undergoing prolonged mechanical ventilation. Luyt CE, Combes A, Deback C, et al. Am J Respir Crit Care Med. 2007;175:935–942. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials