

Role of Spot Urine Sodium in Furosemide Stress Test in Volume-overloaded Critically Ill Patients with Acute Kidney Injury
- PMID: 39759784
- PMCID: PMC11695895
- DOI: 10.5005/jp-journals-10071-24862
Role of Spot Urine Sodium in Furosemide Stress Test in Volume-overloaded Critically Ill Patients with Acute Kidney Injury
Abstract
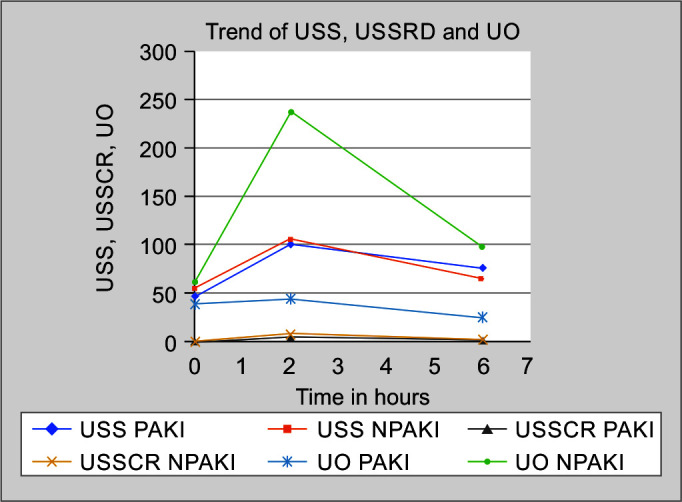
Introduction and aims: Urine output (UO) in response to furosemide stress test (FST) can predict the progression of acute kidney injury (AKI). This study aimed to assess if changes in UO, urine spot sodium (USS), urine spot sodium creatinine ratio (USSCR) and changes in these parameters over 6 hours could differentiate between progressive and non-progressive AKI.
Materials and methods: Fifty critically ill adults with AKI in acute kidney injury network (AKIN) stages I and II with volume overload were included in this prospective study. The FST was performed with 1 mg/kg intravenous bolus. Hourly UO, USS, USSCR, maximum USS difference (USSDMAX), and maximum USSCR difference (USSCRDMAX) were documented. Any progression of AKI was noted till day 3.
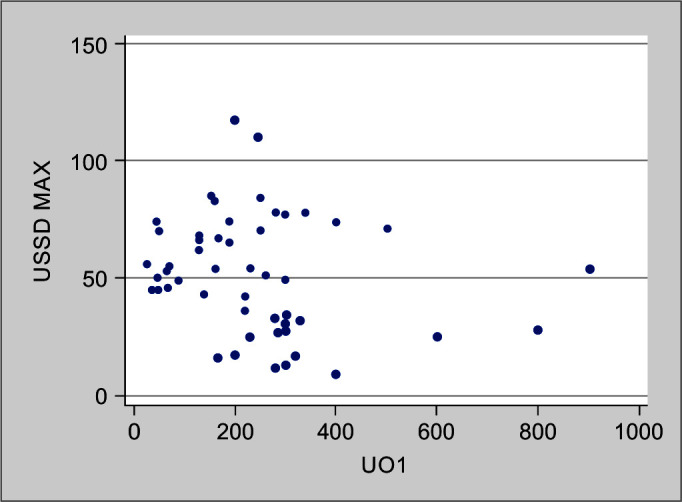
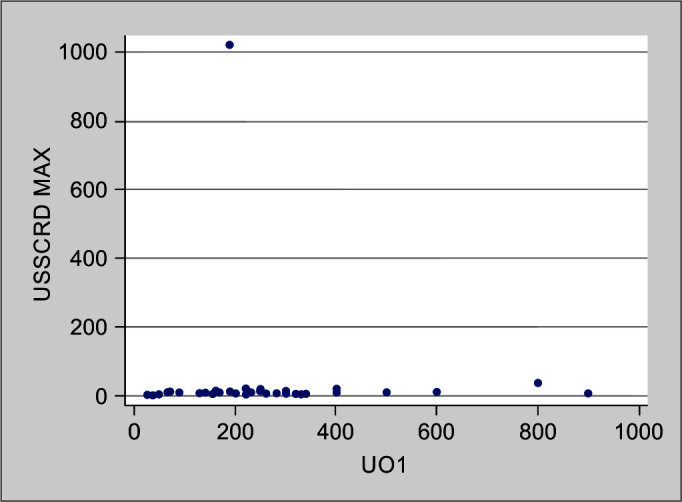
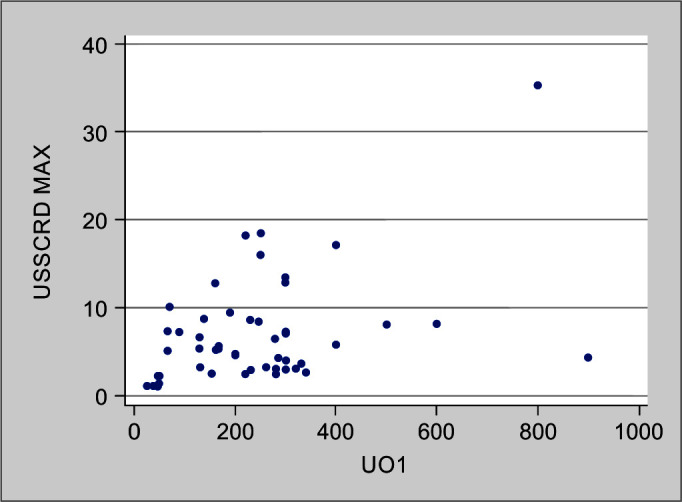
Results: A total of 50 patients were recruited and n = 10 had progressive AKI (PAKI) and n = 40 had non-progressive AKI (NPAKI). Urine output at 1 and 2 h were significantly less in PAKI group. USS0, USS2, USS6, and USSDMAX were comparable between the groups. USSCR0 and USSCR6 were comparable between the groups whereas USSCR2 and USSCRDMAX were significantly less in PAKI group. USSDMAX did not correlate with UO1 (correlation coefficient 0.2, p = 0.16). However, USSCRDMAX showed a poor but significant correlation with UO1 (correlation coefficient 0.3, p = 0.03).
Conclusion: To conclude, hourly UO in the first two hours and maximum change in USSCR within 6 hours following the FST may have an important role in early differentiation of progressive AKI in critically ill patients.
How to cite this article: Suhas P, Anand RK, Baidya DK, Dehran M. Role of Spot Urine Sodium in Furosemide Stress Test in Volume-overloaded Critically Ill Patients with Acute Kidney Injury. Indian J Crit Care Med 2024;28(12):1107-1111.
Keywords: AKI progression; Acute kidney injury; Furosemide stress test; Urine spot sodium; Urine spot sodium creatinine ratio.
Copyright © 2024; The Author(s).
Conflict of interest statement
Source of support: Nil Conflict of interest: NoneConflict of interest: None
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous