

Predictors of sepsis in trauma patients: a National Trauma Data Bank analysis
- PMID: 39760043
- PMCID: PMC11697700
- DOI: 10.3389/fmed.2024.1500201
Predictors of sepsis in trauma patients: a National Trauma Data Bank analysis
Abstract
Background: Trauma remains a global health issue being one of the leading causes of death worldwide. Sepsis and infections are common complications contributing to mortality, emphasizing the need to understand factors leading to such complications following trauma.
Aim: This study aimed to identify risk factors associated with post-trauma sepsis using data from the National Trauma Data Bank (NTDB).
Methods: Using the 2017 National Trauma Data Bank (NTDB), this is a retrospective case-control study that looked at pre-hospital and in-hospital patient data. Trauma patients aged over 15 years presenting to the emergency department (ED) and admitted to a tertiary care center were included. The primary outcome assessed was the development of sepsis post-trauma. Logistic regression analysis was used to identify risk factors, considering patient demographics, injury characteristics, and clinical variables.
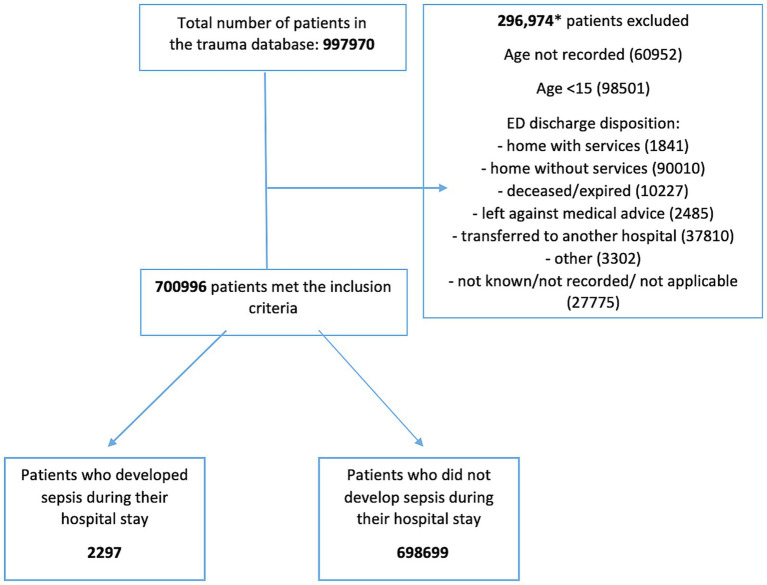
Results: Among 997,970 trauma patients in the 2017 NTDB, 296,974 were excluded, leaving 700,996 patients for analysis, with 2,297 developing sepsis. Patients who developed sepsis were older than those who did not develop sepsis (mean age 57.57 vs. 53.42 years, p-value<0.001) and predominantly white males. Risk factors associated with sepsis development included: respiratory intubation with mechanical ventilation (OR = 11.99; 95% CI = 10.66-13.48), blood transfusion administration (OR = 2.03; 95% CI = 1.83-2.25), Injury Severity Score (ISS) ≥ 16 (OR = 1.69; 95% CI = 1.51-1.89), chronic obstructive pulmonary disease (COPD) (OR = 1.65; 95% CI = 1.44-1.89), diabetes mellitus (DM) (OR = 1.41; 95% CI = 1.26-1.58), male sex (OR = 1.42; 95% CI = 1.28-1.57), hypertension (HTN) (OR = 1.30; 95% CI = 1.16-1.45), anticoagulation therapy (OR = 1.21; 95% CI = 1.05-1.39), older age (OR = 1.02; 95% CI = 1.01-1.02), and current smoking status (OR = 1.18; 95% CI = 1.06-1.32).
Conclusion: This study identified key risk factors for post-trauma sepsis. Recognition of preexisting conditions and injury severity is crucial in trauma patient management to mitigate septic complications. Early identification of at-risk patients could facilitate timely interventions and potentially reduce mortality rates in trauma care settings.
Keywords: Sepsis; injury; mortality; risk factors; trauma.
Copyright © 2024 Bou Chebl, Alwan, Bakkar, Haidar, Bachir, El Sayed and Abou Dagher.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Muckart DJ, Bhagwanjee S. American College of Chest Physicians/Society of Critical Care Medicine consensus conference definitions of the systemic inflammatory response syndrome and allied disorders in relation to critically injured patients. Crit Care Med. (1997) 25:1789–95. doi: 10.1097/00003246-199711000-00014, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources