

Interpretable machine learning for predicting sepsis risk in emergency triage patients
- PMID: 39762406
- PMCID: PMC11704257
- DOI: 10.1038/s41598-025-85121-z
Interpretable machine learning for predicting sepsis risk in emergency triage patients
Abstract
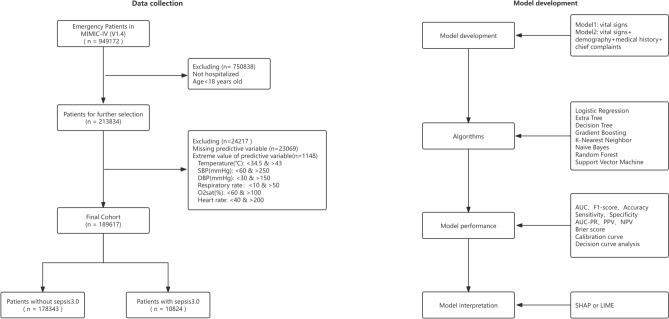
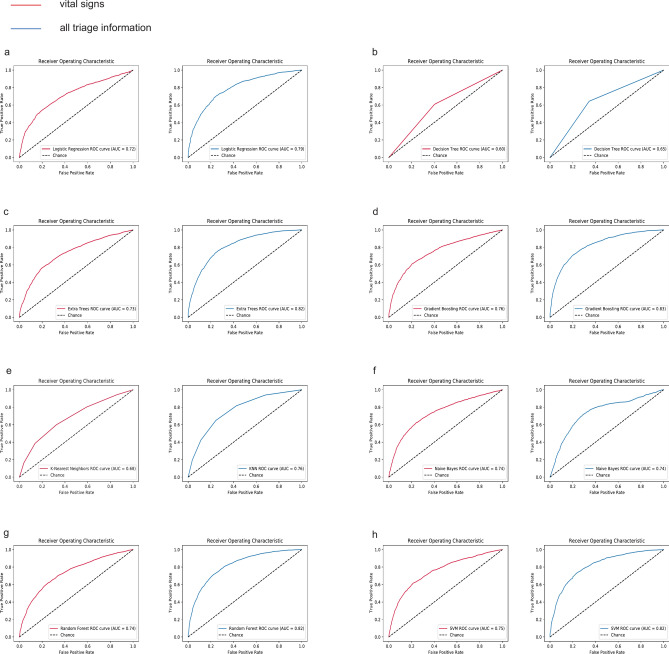
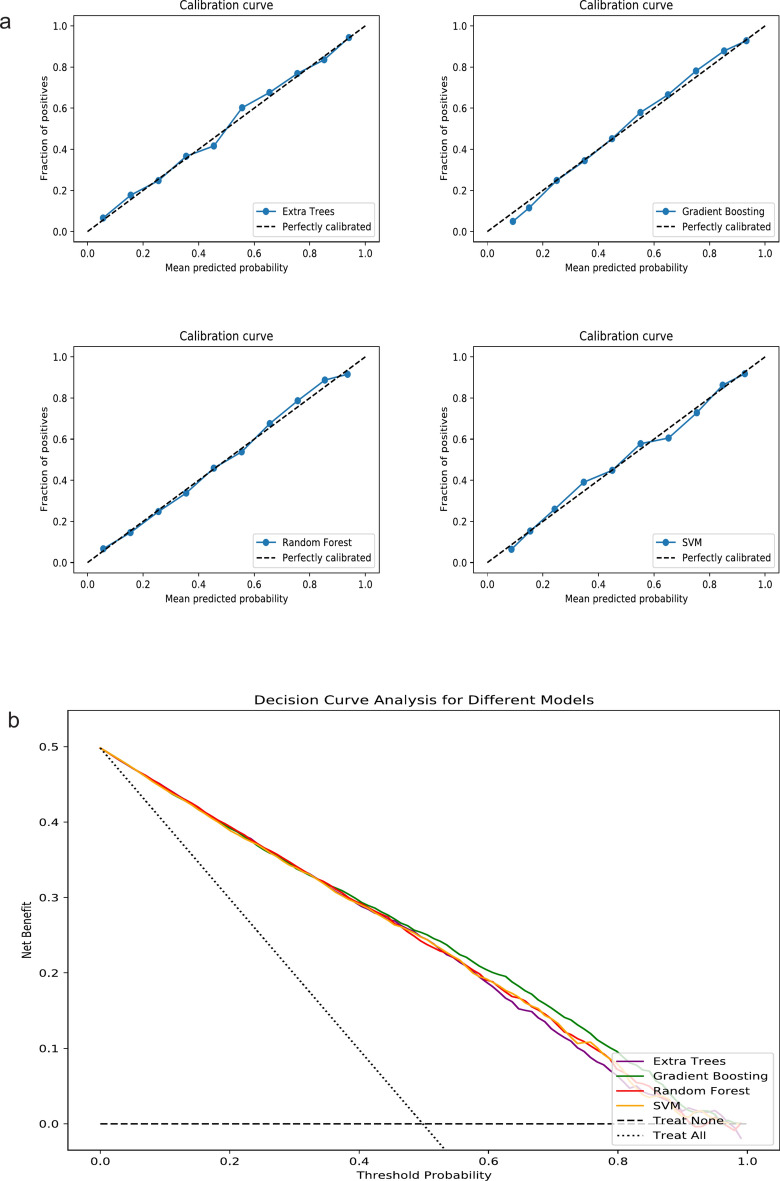
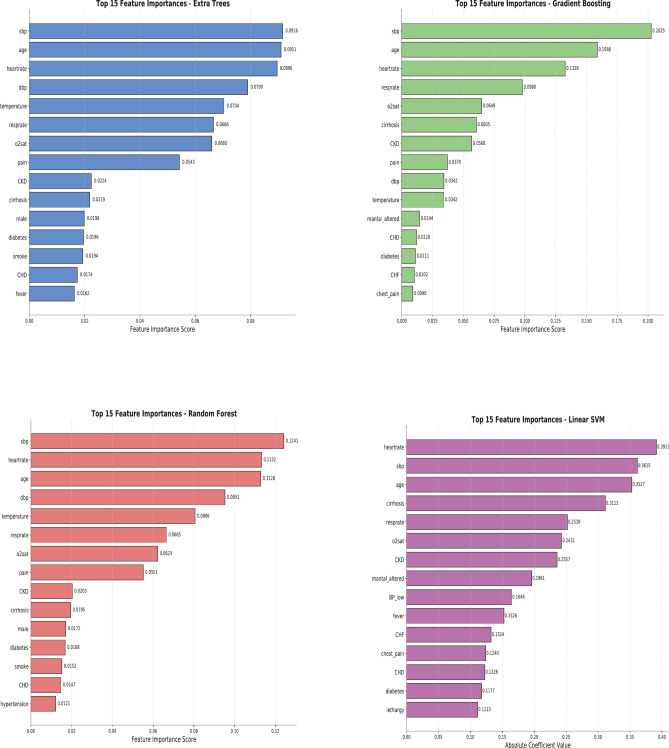
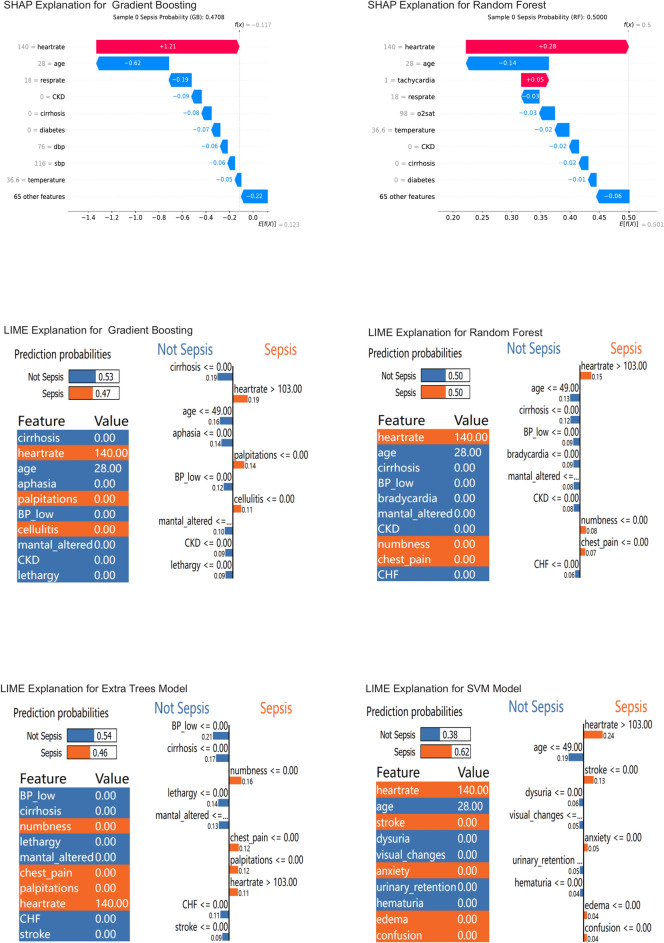
The study aimed to develop and validate a sepsis prediction model using structured electronic medical records (sEMR) and machine learning (ML) methods in emergency triage. The goal was to enhance early sepsis screening by integrating comprehensive triage information beyond vital signs. This retrospective cohort study utilized data from the MIMIC-IV database. Two models were developed: Model 1 based on vital signs alone, and Model 2 incorporating vital signs, demographic characteristics, medical history, and chief complaints. Eight ML algorithms were employed, and model performance was evaluated using metrics such as AUC, F1 Score, and calibration curves. SHapley Additive exPlanations (SHAP) and Local Interpretable Model-agnostic Explanations (LIME) methods were used to enhance model interpretability. The study included 189,617 patients, with 5.95% diagnosed with sepsis. Model 2 consistently outperformed Model 1 across most algorithms. In Model 2, Gradient Boosting achieved the highest AUC of 0.83, followed by Extra Tree, Random Forest, and Support Vector Machine (all 0.82). The SHAP method provided more comprehensible explanations for the Gradient Boosting algorithm. Modeling with comprehensive triage information using sEMR and ML methods was more effective in predicting sepsis at triage compared to using vital signs alone. Interpretable ML enhanced model transparency and provided sepsis prediction probabilities, offering a feasible approach for early sepsis screening and aiding healthcare professionals in making informed decisions during the triage process.
Keywords: Emergency; Interpretable machine learning; Sepsis; Triage; Warning mode.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics declarations: The data for this study came from a public database. The study design was approved by the appropriate ethics review board. Informed consent was not necessary because the database used was anonymized.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
