

Autogene cevumeran with or without atezolizumab in advanced solid tumors: a phase 1 trial
- PMID: 39762422
- PMCID: PMC11750724
- DOI: 10.1038/s41591-024-03334-7
Autogene cevumeran with or without atezolizumab in advanced solid tumors: a phase 1 trial
Abstract
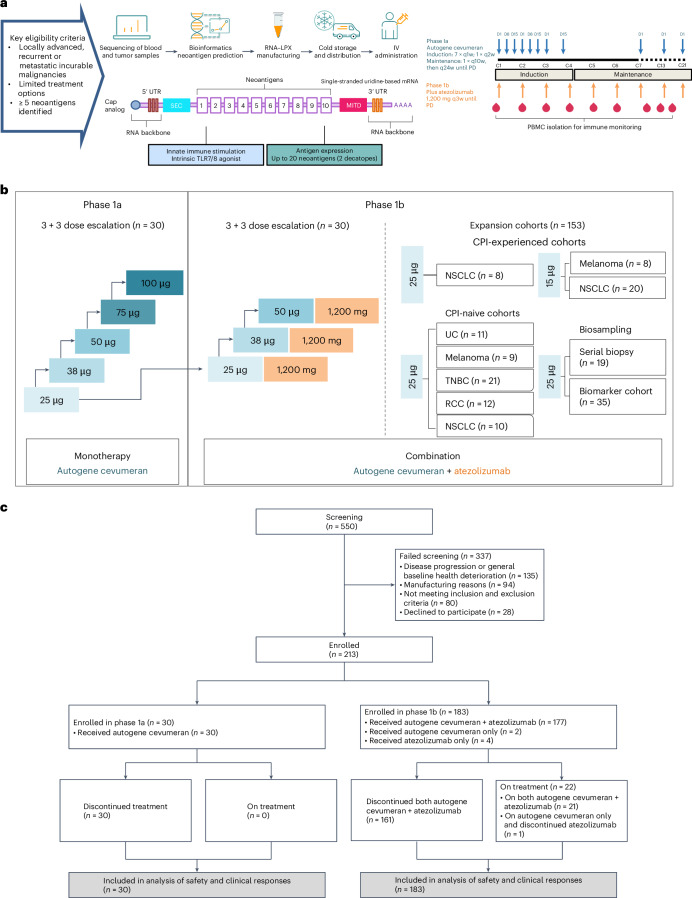
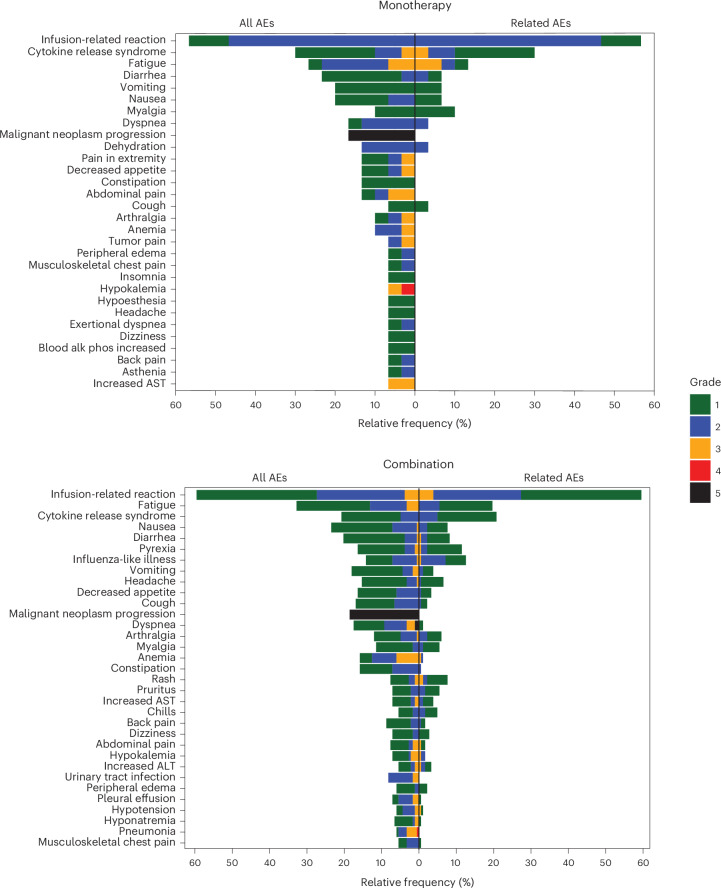
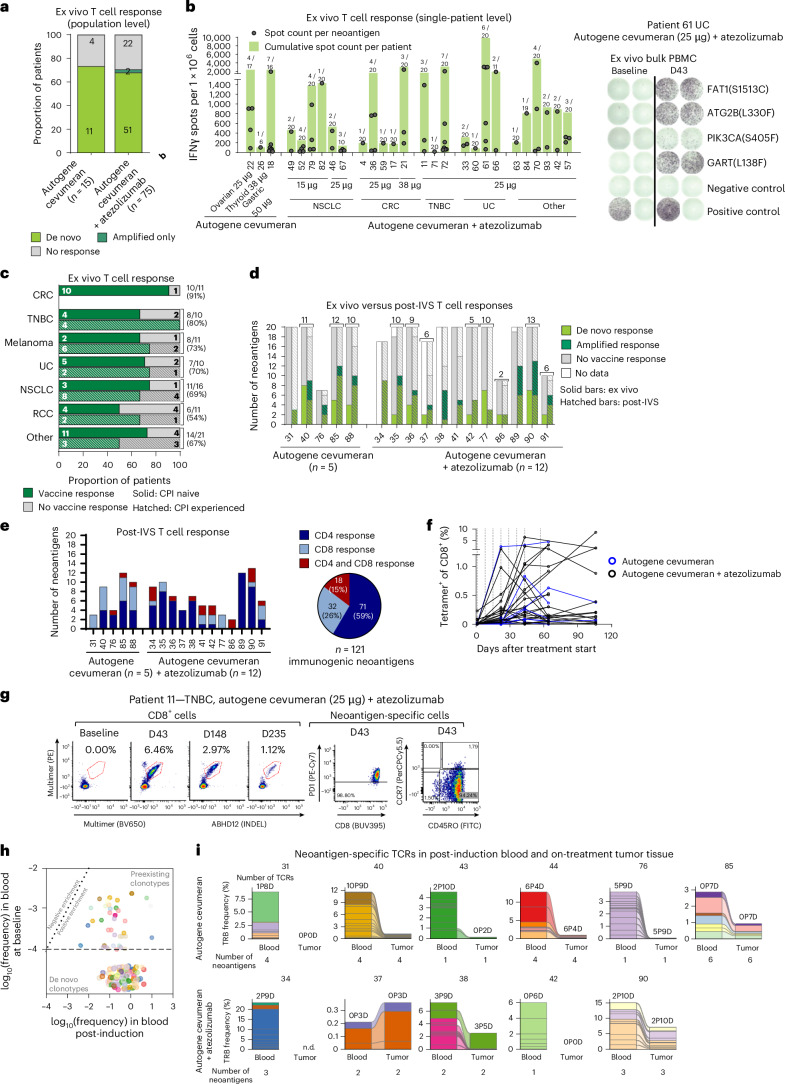
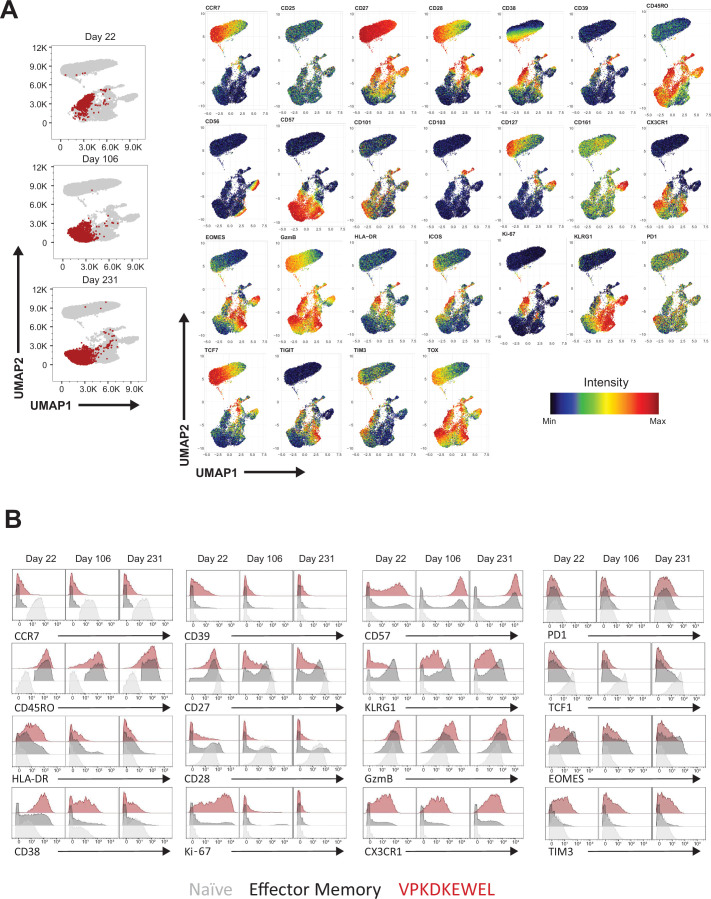
Effective targeting of somatic cancer mutations to enhance the efficacy of cancer immunotherapy requires an individualized approach. Autogene cevumeran is a uridine messenger RNA lipoplex-based individualized neoantigen-specific immunotherapy designed from tumor-specific somatic mutation data obtained from tumor tissue of each individual patient to stimulate T cell responses against up to 20 neoantigens. This ongoing phase 1 study evaluated autogene cevumeran as monotherapy (n = 30) and in combination with atezolizumab (n = 183) in pretreated patients with advanced solid tumors. The primary objective was safety and tolerability; exploratory objectives included evaluation of pharmacokinetics, pharmacodynamics, preliminary antitumor activity and immunogenicity. Non-prespecified interim analysis showed that autogene cevumeran was well tolerated and elicited poly-epitopic neoantigen-specific responses, encompassing CD4+ and/or CD8+ T cells, in 71% of patients, most of them undetectable at baseline. Responses were detectable up to 23 months after treatment initiation. CD8+ T cells specific for several neoantigens constituted a median of 7.3% of circulating CD8+ T cells, reaching up to 23% in some patients. Autogene cevumeran-induced T cells were found within tumor lesions constituting up to 7.2% of tumor-infiltrating T cells. Clinical activity was observed, including one objective response in monotherapy dose escalation and in two patients with disease characteristics unfavorable for response to immunotherapy treated in combination with atezolizumab. These findings support the continued development of autogene cevumeran in earlier treatment lines. ClinicalTrials.gov registration: NCT03289962 .
© 2025. Genentech, Inc. and the Author(s).
Conflict of interest statement
Competing interests: J.L. reports research funding to their institution from Roche-Genentech, Basilea, Astex, Merck, GSK, Eisai, Seagen, Immunocore, BicycleTx, AstraZeneca, Genmab, Bayer, Jansenn, Gilead, Anaveon, Affimed, Appollomics, Avacta, Byondis, Chugai, CellCentric, Daiichi, Iteos, Merck Serono, REDX, and Amgen, and a consulting and advisory role for Basilea, Roche-Genentech, Ellipses, Eisai, Pierre-Faber and GSK. T.P. reports a consulting and advisory role for Astellas Pharma, Bristol Myers Squibb, Exelixis, Incyte, Ipsen, Johnson & Johnson, Mashup Ltd, Merck Serono, MSD, Novartis, Pfizer, Roche and Seattle Genetics; travel, accommodation or expenses from Ipsen, MSD, Pfizer and Roche; and research funding from Astellas Pharma, Bristol Myers Squibb, Exelixis, Ipsen, Johnson & Johnson, Merck Serono, MSD, Novartis, Pfizer, Roche, Seattle Genetics. F.B. reports speaking engagements and advisory boards for Roche/Genentech, BMS, Lilly, EMD Serono, AstraZeneca and Regeneron, Merck, Seagen, Jazz Pharmaceuticals, Taiho, Incyte Deciphera and Astellas. L.L.S. reports a consulting and advisory role for Merck, Pfizer, AstraZeneca, Roche, GlaxoSmithKline, Voronoi, Arvinas, Navire, Relay, Daiichi Sankyo, Coherus, Amgen, Marengo, Medicenna, Tubulis, LTZ Therapeutics and Pangea; grants or support for clinical trials to their institution from Novartis, Bristol Myers Squibb, Pfizer, Boerhinger-Ingelheim, GlaxoSmithKline, Roche/Genentech, AstraZeneca, Merck, Celgene, Astellas, Bayer, Abbvie, Amgen, Symphogen, Mirati, BioNTech, 23Me and EMD Serono; stock ownership (spouse) of Agios; and leadership (spouse) at Treadwell Therapeutics. P.L. has served on the advisory boards of Abbvie, GenMab, Genentech, CytomX, Takeda, Cybrexa, Agenus, IQVIA, TRIGR, Pfizer, ImmunoMet, Black Diamond, GSK, QED Therapeutics, AstraZeneca, EMD Serono, Shattuck, Astellas, Salarius, Silverback, MacroGenics, Kyowa Kirin Pharmaceutical Development, Kineta, Inc, Zentalis Pharmaceuticals, Molecular Templates, STCube Pharmaceuticals, Bayer, I-Mab, Seagen, imCheck, Relay Therapeutics, Stemline, Compass BADX, Mekanist, Mersana Therapeutics, BAKX Therapeutics, Scenic Biotech, Qualigen, NeuroTrials and Actuate Therapeutics; on the data safety monitoring board for Agios, Five Prime, Halozyme and Tyme; and as a consultant for Roche-Genentech, SOTIO, SK Life Science and Roivant Sciences. C.F.F. reports a consulting and advisory role (self) for Seagen, Aadi Biosciences, Genentech/MyPathway (uncompensated) and Merck/LYNK-002 (uncompensated), and institutional funding from Bristol Myers Squibb, Daiichi, Hotspot Therapeutics, Marengo, AstraZeneca, Genentech/Roche, Immunocore, Seagen and Merck. A.S.B. reports serving on a speakers bureau for Genentech, BMS, Mirati, AstraZeneca, Regeneron and Merck and consulting for Pfizer and Abbvie, and is on a steering committee for Janssen. M.G. reports clinical trial support to their institution from Genentech/Roche, GSK, Abbvie, Merck Serono, Medimmune, Incyte, Pfizer, Amgen, Gilead Sciences, Zai Labs, Adanate, Fog Pharma, PEEL, Orionis, SQZ, YMABS, Iovance, Vincerx, Werewolf, Endocyte, Seattle Genetics, Plexxicon/Daiichi, Celldex, Tracon, Deciphera, Fujifilm, Minnemarita, Nektar, Novita, Biosplice, Corcept, Novartis, Toray, Genzada, Salarius, Agenus, Inhibrx, AADI, Revolution Medicine, Blueprint, Astellas, BioNTech, Helix, IgM Biosciences, ImmuneSensor, Bioeclipse, Bioline, Black Diamond, Codiak, Dracen, Elevation Oncology, Famewave, Forma Therapeutics, IntraImmun SG, Pionyr, Trishula, Tolero, Vedanta Biosciences, Coordination Therapeutics, Ideaya Biosciences, I-Mab, NiKang, Nimbus Therapeutics, OncoResponse, Riboscience, Rubius Therapeutics, Simcha Therapeutics, Siranomics, Synthorx and Theseus Pharmaceuticals; consulting fees from Pfizer, Imaging Endpoints and Curio; honoraria from Lisa Stearns Academy; a patent with Sphinx Health Solutions; and advisory boards for Daiichi, Qualigen, Springworks, Cardinal Healthcare, IQVIA and Medtronics. I.K. reports consulting fees from and serving in a speakers bureau for Delcath Inc., Immunocore Ltd and Pierre Fabre Inc; educational grants from BMS and Novartis; and travel grants from Delcath Inc, Genentech Inc, BMS and Merck Serono. G.A.F. reports serving on a data safety monitoring board for AstraZeneca and Hutchison Pharma and advisory boards for Bristol Myers Squibb and Merck. M. Schmidt reports personal fees from AstraZeneca, BioNTech, Daiichi Sankyo, Eisai, Lilly, MSD, Novartis, Pantarhei Bioscience, Pfizer, Pierre Fabre, Roche and SeaGen outside the submitted work; institutional research funding from AstraZeneca, BioNTech, Eisai, Genentech, German Breast Group, Novartis, Palleos, Pantarhei Bioscience, Pierre Fabre and SeaGen; and a patent for EP 2390370 B1 filed for EP 2951317 B1 filed. M. Schuler received consulting fees from Amgen, AstraZeneca, Blueprint Medicines, Boehringer Ingelheim, Bristol Myers Squibb, GlaxoSmithKline, Janssen, Merck Serono, Novartis, Roche, Sanofi, Takeda and Tacalyx; honoraria from Amgen, Bristol Myers Squibb, Janssen, MSD, Novartis, Roche and Sanofi; and research funding to their institution from AstraZeneca, Bristol Myers Squibb and Janssen. R.J.S. served as a consultant and in advisory boards for Marengo, Merck, Novartis, Pfizer and Replimune and has received research funding to their institution from Merck. H.B. reports research funding to their institution from AbbVie, Agios, ARMO Biosciences, Array BioPharma, Arvinas, AstraZeneca, Bayer, BeiGene, BioAtla, BioMed Valley Discoveries, BioTheryX, Boehringer Ingelheim, Bristol Myers Squibb, CALGB, Celgene, CicloMed, Coordination Pharmaceuticals, eFFECTOR Therapeutics, Lilly, EMD Serono, Roche/Genentech, GlaxoSmithKline, Gossamer Bio, Harpoon Therapeutics, Hengrui Therapeutics, Incyte, Janssen, Jounce Therapeutics, Kymab, MacroGenics, MedImmune, Merck, Millennium/Takeda, Moderna, NGM Biopharmaceuticals, Novartis, Pfizer, Revolution Medicines, Ryvu Therapeutics, Foundation Medicine, SeaGen, Tesaro, TG Therapeutics, Verastem, Vertex Pharmaceuticals, Xbiotech and Zymeworks; consulting (uncompensated) for Bristol Myers Squibb, Novartis and TG Therapeutics; consulting (payments to institution) for AstraZeneca, GRAIL, Incyte, Roche and Vincerx Pharma; and stock ownership in HCA Healthcare. V.G. reports institutional support from Seagen Inc., SOTIO Biotech AG, Shattuck Labs, Inc., T-knife GmbH, F. Hoffmann-La Roche Ltd, Janssen Research & Development, LLC, Novartis, Affimed GmbH, Anaveon AG, BioNTech SE, BicycleTx Ltd, Epizyme, Inc., Regeneron Pharmaceuticals, Inc., Boehringer Ingelheim, Genmab, Pieris Pharmaceuticals, Inc., Celgene Corporation, Debiopharm International S.A., F-star Therapeutics Limited, ImCheck Therapeutics, Gilead Sciences, Inc and Sanofi-Aventis Recherche & Développement. B.S.H. reports a consulting and advisory role for AstraZeneca, Ideaya, Jazz Pharmaceuticals, Sorrento Therapeutics, Genentech-Roche, OncLive, Veeva, Athenium, Boxer Capital, SAI-Med and DAVA Oncology, and research funding to their institution from NexImmune, Genentech-Roche, Johnson & Johnson, BMS Foundation/VCU, Stand Up 2 Cancer, V Foundation and National Cancer Institute. P.A.O. reports consulting for Array, Bristol Myers Squibb, Celldex, CytomX, Evaxion, Genentech, Imunon, Merck, MyNEO, Neon Therapeutics, Novartis, Pfizer, Phio, TRM Oncology and Servier, and grant and research support to their institution from Agenus, AstraZeneca/MedImmune, Bristol Myers Squibb, Celldex, CytomX, Genentech, Merck, Neon Therapeutics, Novartis and Pfizer. G.J. received consulting fees from Novartis, Amgen, Roche, Pfizer, Bristol Myers Squibb, Lilly, AstraZeneca, Daiichi Sankyo, Abbvie, Seagen and Diaccurate; honoraria from Novartis, Amgen, Roche, Pfizer, Bristol Myers Squibb, Lilly, AstraZeneca, Daiichi Sankyo, Abbvie and Seagen; and travel support from Novartis, Roche, Pfizer, Lilly, Amgen, Bristol Myers Squibb and AstraZeneca; served on a board for Novartis, Roche, Pfizer, Lilly, Amgen, Bristol Myers Squibb and AstraZeneca; and received materials or services from Novartis, Roche, Lilly, Amgen, Bristol Myers Squibb and AstraZeneca. L.F. reports research support from Abbvie, Bavarian Nordic, Bristol Myers Squibb, Dendreon, Janssen, Merck and Roche/Genentech, and ownership interests in Actym, Atreca, Bioatla, Bolt, Immunogenesis, Nutcracker, RAPT, Scribe and Senti. N.S. provided consultation or attended advisory boards for Boehringer Ingelheim, Ellipses Pharma, GlaxoSmithKline, Incyte and Luszana, and received research grants from Abbvie, Actuate Therapeutics, Amgen, Array, Ascendis Pharma, AstraZeneca, Bayer, Blueprint Medicines, Boehringer Ingelheim, BridgeBio, Bristol Myers Squibb, Cantargia, CellCentric, Cogent Biosciences, Cresecendo Biologics, Cytovation, Deciphera, Dragonfly, Eli Lilly, Exelixis, Genentech, GlaxoSmithKline, IDRx, Immunocore, Incyte, InteRNA, Janssen, Kinnate Biopharma, Kling Biotherapeutics, Lixte, Luszana, Merck, Merck Sharp & Dohme, Merus, Molecular Partners, Navire Pharma, Novartis, Numab Therapeutics, Pfizer, Relay Pharmaceuticals, Revolution Medicin, Roche, Sanofi, Seattle Genetics, Taiho and Takeda (all outside the submitted work; payment was made to the Netherlands Cancer Institute). R.S.L. reports research and grant funding from Bristol Myers Squibb, Clinigen, Celldex, Incyte and Ubivac, and consulting and advisory roles for Bristol Myers Squibb, Merck, CDR-Life and Vir. A.R. was a consultant and advisor for AbbVie, AstraZeneca, BMS, Boehringer Ingelheim, Daichi Sankyo, Eli Lilly, GSK, MSD, Novartis, Pfizer and Roche/Genentech. S.A.L. reports funding to their institution from Roche/Genentech. R.A. is a primary investigator on S1933 (atezolizumab). I. Melero reports grants from Roche, BMS, Genmab and AstraZeneca, and was a consultant for Roche, BMS, Genmab, AstraZeneca, Biontech, Pharmamar, F-Star, Numab, Mestag, Curon and Bright Peaks. R.L.S., I.R., M.R.M., L. Muller, G.D.F., M.Y., L.K., V.J.P.L., A.R., M.D., T.Q., J. Zhu, J. Zhang, P.T., G.K.R., D.W.L., C.P., A.A.L., J.M.S., L.D. and I. Mellman are or were employees of Genentech, Inc. and are or were Roche stockholders. L. Muller is now an employee and shareholder of Gilead Sciences. G.D.F. reports stock ownership in CARGO Therapeutics. F.M., E.D., A.C., L. Manning, D.M., S.B., V.L., T.O., E.G., D.B., C.H., C.W., C.A., C.K., A.D.T., J.D., M.V., A.J., A.P., J.B., O.H., A.N.K., U.S. and Ö.T. are employees of BioNTech, a company developing immunotherapies against cancer and other diseases, and may hold securities in the company. U.S. and Ö.T. are management board members of BioNTech SE (Mainz, Germany). M.L., M.V., A.D.T., J.D., A.N.K., U.S. and Ö.T. are co-authors on various issued or pending patents that cover parts of this Article. D.R.C. served on advisory boards and consulted for Roche/Genentech. J.Y., S.R., L.D., D.J., K.M.W., A.S. and E.G. report no competing interests.
Figures









References
-
- Sharma, P. et al. Immune checkpoint therapy—current perspectives and future directions. Cell186, 1652–1669 (2023). - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
