

Burdens of type 2 diabetes and cardiovascular disease attributable to sugar-sweetened beverages in 184 countries
- PMID: 39762424
- PMCID: PMC11835746
- DOI: 10.1038/s41591-024-03345-4
Burdens of type 2 diabetes and cardiovascular disease attributable to sugar-sweetened beverages in 184 countries
Erratum in
-
Author Correction: Burdens of type 2 diabetes and cardiovascular disease attributable to sugar-sweetened beverages in 184 countries.Nat Med. 2025 Feb;31(2):696. doi: 10.1038/s41591-025-03524-x. Nat Med. 2025. PMID: 39870818 Free PMC article. No abstract available.
Abstract
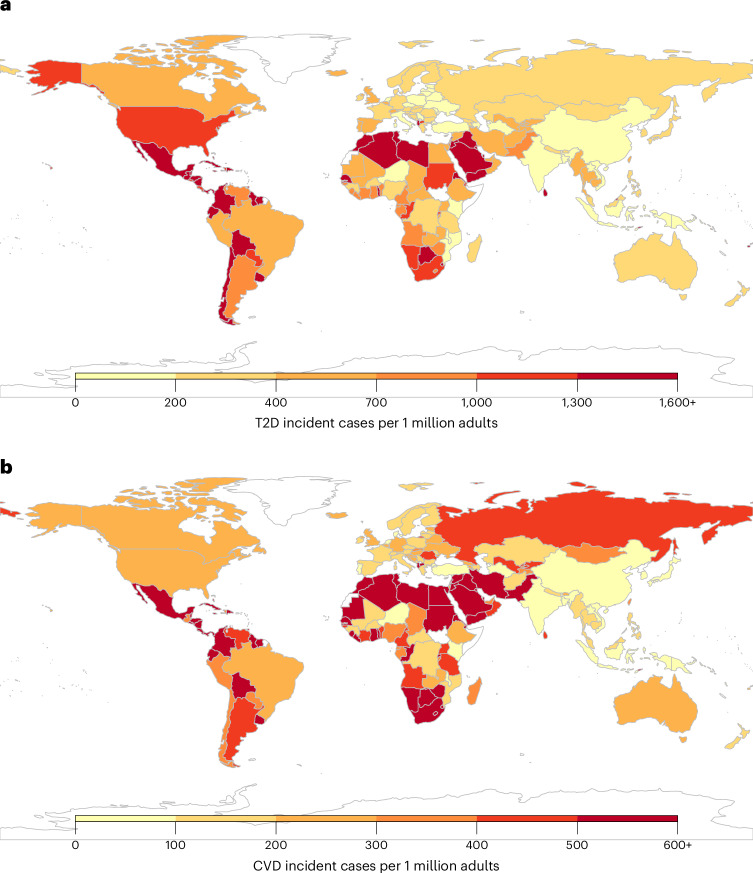
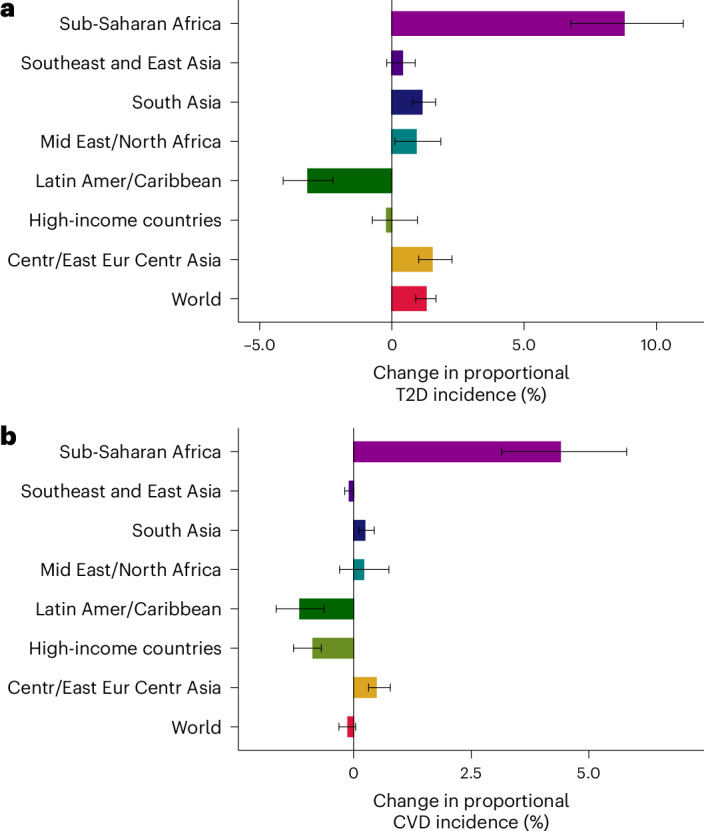
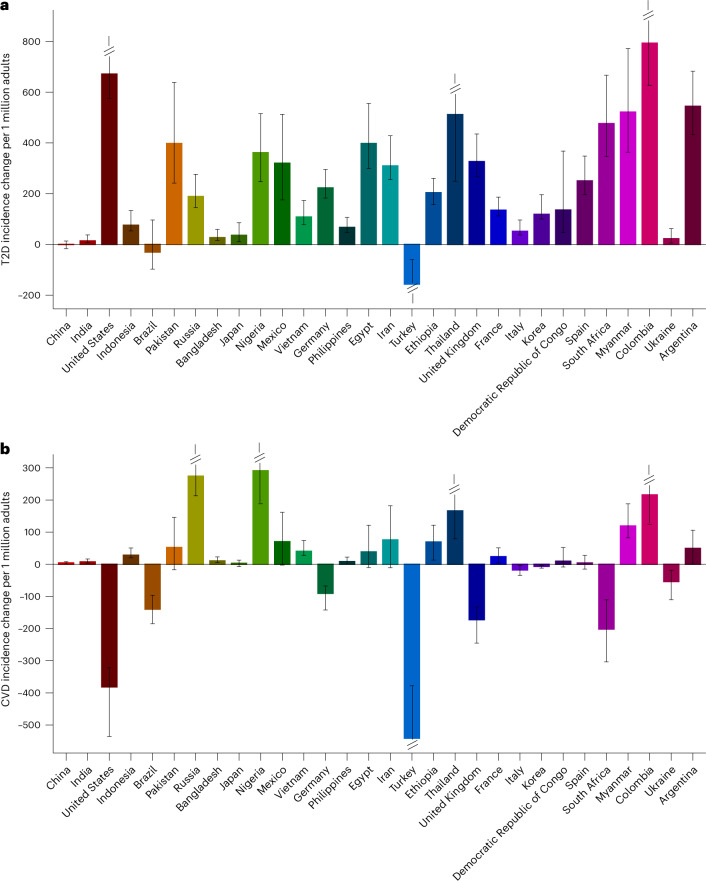
The consumption of sugar-sweetened beverages (SSBs) is associated with type 2 diabetes (T2D) and cardiovascular diseases (CVD). However, an updated and comprehensive assessment of the global burden attributable to SSBs remains scarce. Here we estimated SSB-attributable T2D and CVD burdens across 184 countries in 1990 and 2020 globally, regionally and nationally, incorporating data from the Global Dietary Database, jointly stratified by age, sex, educational attainment and urbanicity. In 2020, 2.2 million (95% uncertainty interval 2.0-2.3) new T2D cases and 1.2 million (95% uncertainty interval 1.1-1.3) new CVD cases were attributable to SSBs worldwide, representing 9.8% and 3.1%, respectively, of all incident cases. Globally, proportional SSB-attributable burdens were higher among men versus women, younger versus older adults, higher- versus lower-educated adults, and adults in urban versus rural areas. By world region, the highest SSB-attributable percentage burdens were in Latin America and the Caribbean (T2D: 24.4%; CVD: 11.3%) and sub-Saharan Africa (T2D: 21.5%; CVD: 10.5%). From 1990 to 2020, the largest proportional increases in SSB-attributable incident T2D and CVD cases were in sub-Saharan Africa (+8.8% and +4.4%, respectively). Our study highlights the countries and subpopulations most affected by cardiometabolic disease associated with SSB consumption, assisting in shaping effective policies and interventions to reduce these burdens globally.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The investigators did not receive funding from a pharmaceutical company or other agency to write this report. L.L.-C. reports research funding from the Gates Foundation, the American Heart Association and Consejo Nacional de Ciencia y Tecnología in Mexico (CONACyT), outside of the submitted work. M.O. reports previous research funding from the Gates Foundation, as well as the National Institutes of Health and employment with Food Systems for the Future, outside of the submitted work. R.M. reports research funding from the Gates Foundation and (ended) the US National Institutes of Health, Danone and Nestle. She also reports consulting from Development Initiatives and as IEG chair for the Global Nutrition Report, outside of the submitted work. F.C., J.Z. and P.S. report research funding from the Gates Foundation, as well as the National Institutes of Health, outside of the submitted work. V.M. reports research funding from the Canadian Institutes of Health Research and from the American Heart Association, outside the submitted work. J.R.S. reports research funding from the Gates Foundation, as well as the National Institutes of Health, Nestlé, Rockefeller Foundation and Kaiser Permanent Fund at East Bay Community Foundation, outside of the submitted work. S.B. reports funding from Bloomberg Philanthropies, CONACyT, United Nations International Children’s Emergency Fund (UNICEF) and Fundación Rio Arronte, all outside the submitted work. S.B.C. reports research funding from the US National Institutes of Health, US Department of Agriculture, the Rockefeller Foundation, US Agency for International Development and the Kaiser Permanente Fund at East Bay Community Foundation, outside the submitted work. D.M. reports research funding from the US National Institutes of Health, the Gates Foundation, the Rockefeller Foundation, the Kaiser Permanente Fund at East Bay Community Foundation and the National Association of Chain Drug Stores Foundation; scientific advisory board membership for Beren Therapeutics, Brightseed, Calibrate, Elysium Health, HumanCo, Instacart, January Inc., Season Health and the Validation Institute; equity in Calibrate and HumanCo; and chapter royalties from UpToDate, all outside the submitted work.
Figures






References
-
- Beal, T., Herforth, A., Sundberg, S., Hess, S. Y. & Neufeld, L. M. Differences in modelled estimates of global dietary intake. Lancet397, 1708–1709 (2021). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
