

Prediction of checkpoint inhibitor immunotherapy efficacy for cancer using routine blood tests and clinical data
- PMID: 39762425
- PMCID: PMC11922749
- DOI: 10.1038/s41591-024-03398-5
Prediction of checkpoint inhibitor immunotherapy efficacy for cancer using routine blood tests and clinical data
Abstract
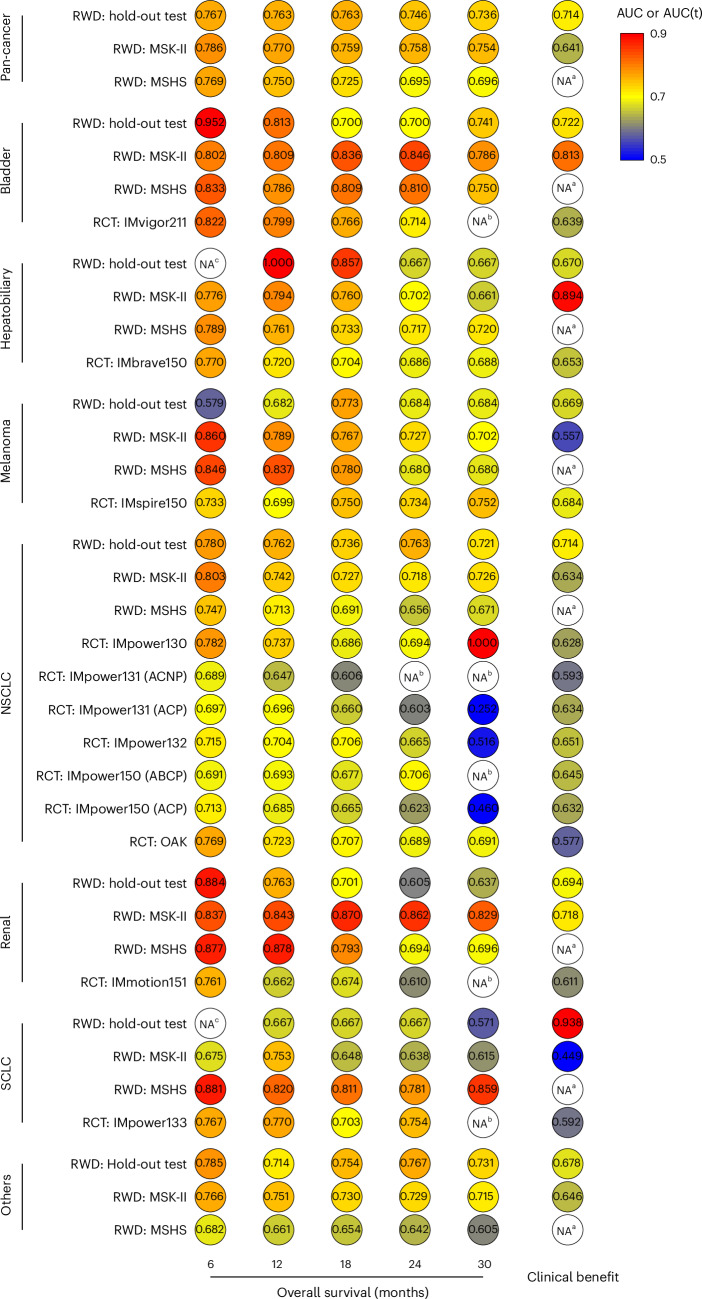
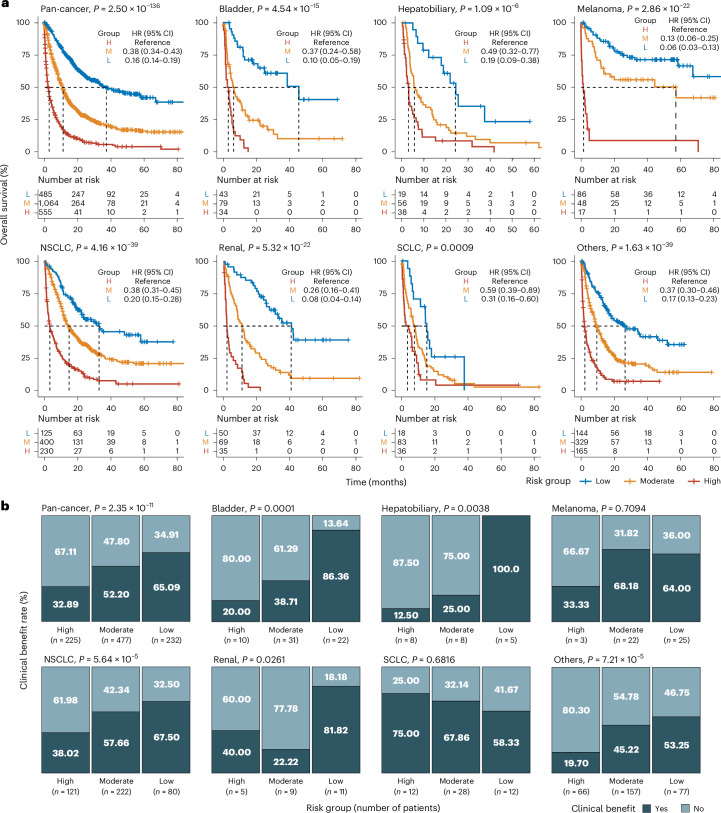
Predicting whether a patient with cancer will benefit from immune checkpoint inhibitors (ICIs) without resorting to advanced genomic or immunologic assays is an important clinical need. To address this, we developed and evaluated SCORPIO, a machine learning system that utilizes routine blood tests (complete blood count and comprehensive metabolic profile) alongside clinical characteristics from 9,745 ICI-treated patients across 21 cancer types. SCORPIO was trained on data from 1,628 patients across 17 cancer types from Memorial Sloan Kettering Cancer Center. In two internal test sets comprising 2,511 patients across 19 cancer types, SCORPIO achieved median time-dependent area under the receiver operating characteristic curve (AUC(t)) values of 0.763 and 0.759 for predicting overall survival at 6, 12, 18, 24 and 30 months, outperforming tumor mutational burden (TMB), which showed median AUC(t) values of 0.503 and 0.543. Additionally, SCORPIO demonstrated superior predictive performance for predicting clinical benefit (tumor response or prolonged stability), with AUC values of 0.714 and 0.641, compared to TMB (AUC = 0.546 and 0.573). External validation was performed using 10 global phase 3 trials (4,447 patients across 6 cancer types) and a real-world cohort from the Mount Sinai Health System (1,159 patients across 18 cancer types). In these external cohorts, SCORPIO maintained robust performance in predicting ICI outcomes, surpassing programmed death-ligand 1 immunostaining. These findings underscore SCORPIO's reliability and adaptability, highlighting its potential to predict patient outcomes with ICI therapy across diverse cancer types and healthcare settings.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: S.-K.Y., B.A.C., C.W.F., C.H., L.G.T.M. and D.C. have a provisional patent application for using routine blood tests and clinical variables to predict cancer immunotherapy response. D.C., R.M.S. and L.G.T.M. are co-inventors on a patent (US11230599/EP4226944A3) filed by MSKCC for using TMB to predict immunotherapy response, licensed to Personal Genome Diagnostics (PGDx). S.-K.Y., C.V., L.G.T.M. and D.C. are co-inventors on a patent (US20240282410A1) filed jointly by Cleveland Clinic and MSKCC for a multi-modal machine learning model to predict immunotherapy response, licensed to Tempus. S.G. reports grants from Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Genentech, Regeneron and Takeda not related to this study and personal fees from Taiho outside the submitted work. M.D.G reports grants from Bristol Myers Squibb, AstraZeneca, Merck and Genentech, and serves as an advisory board/consultant for Astellas, Bristol Myers Squibb, Merck, Genentech, AstraZeneca, Pfizer, EMD Serono, SeaGen, Janssen, Numab, Dragonfly, GlaxoSmithKline, Basilea, UroGen, Rappta Therapeutics, Alligator, Silverback, Fujifilm, Curis, Gilead, Bicycle, Asieris, Abbvie, Analog Devices, Veracyte, Daiichi and Aktis. E.E.S is an executive officer at Pathos, a clinical-stage oncology drug development and information company, and owns equity in this company. The other authors declare no competing interests.
Figures




References
-
- Subbiah, V., Solit, D. B., Chan, T. A. & Kurzrock, R. The FDA approval of pembrolizumab for adult and pediatric patients with tumor mutational burden (TMB) ≥10: a decision centered on empowering patients and their physicians. Ann. Oncol.31, 1115–1118 (2020). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
