

To intubate or to resuscitate: the effect of simulation-based training on advanced airway management during simulated paediatric resuscitations
- PMID: 39762959
- PMCID: PMC11705721
- DOI: 10.1186/s41077-024-00326-y
To intubate or to resuscitate: the effect of simulation-based training on advanced airway management during simulated paediatric resuscitations
Abstract
Background: We aimed to measure the effect of a 2-day structured paediatric simulation-based training (SBT) on basic and advanced airway management during simulated paediatric resuscitations.
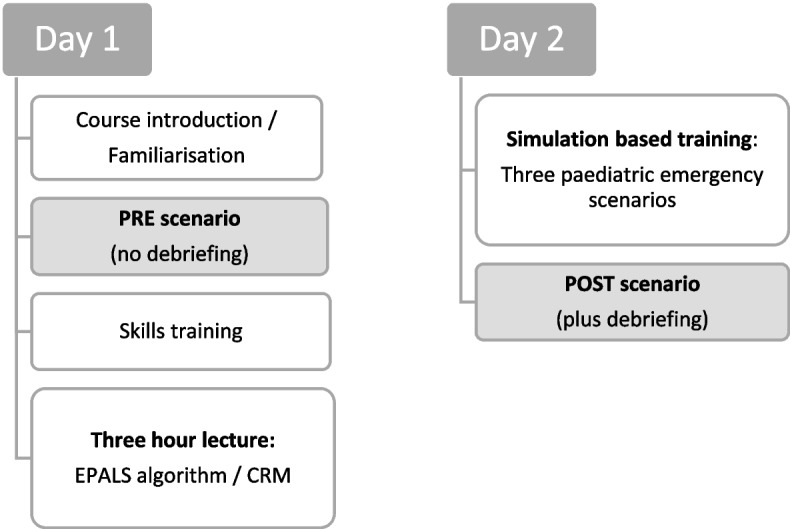
Methods: Standardised paediatric high-fidelity SBT was conducted in 12 of the 15 children's hospitals in Hesse, Germany. Before and after the SBT the study participants took part in two study scenarios (PRE and POST scenario), which were recorded using an audio-video system. Airway management was assessed using a performance evaluation checklist. Time to initiate ventilation, frequency, and timing of endotracheal intubation (ETI), and its influence on other life support interventions were assessed. Differences in airway management between hospitals with and without a PICU were evaluated.
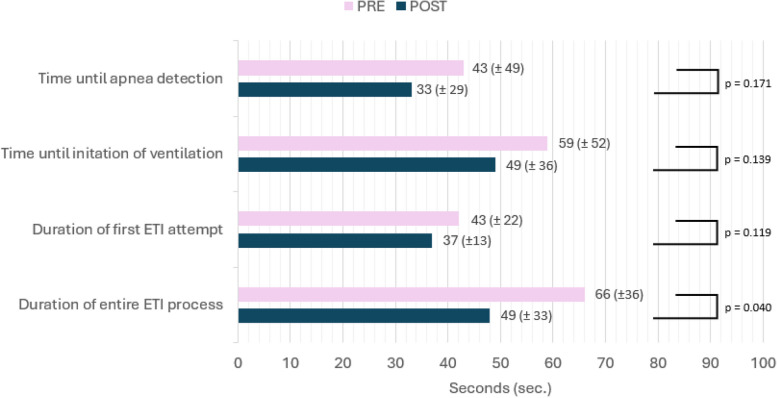
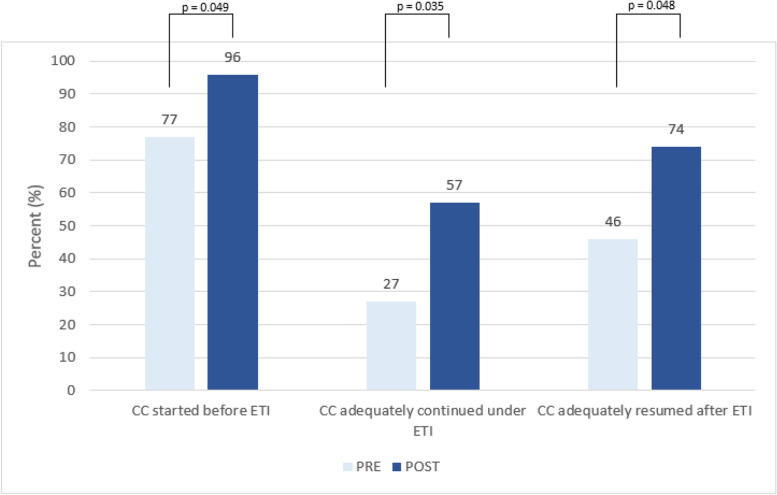
Results: Two hundred twenty-nine participants formed 58 interprofessional resuscitation teams. All teams recognised apnoea in their simulated patients and initiated ventilation during the scenarios. Time to recognition of apnoea and time to initiation of ventilation did not improve significantly after SBT, but teams were significantly more likely to select appropriately sized airway equipment. ETI was attempted in 55% PRE and 40% POST scenarios (p=0.1). The duration of the entire ETI process was significantly shorter in the POST scenarios. Chest compressions (CC) were frequently discontinued during ETI attempts, which improved after SBT (PRE 73% vs. POST 43%, p = 0.035). Adequate resumption of CC after completion of intubation was also significantly more frequent in the POST scenarios (46% vs. 74%, p = 0.048). During ETI attempts, CC were more likely to be adequately continued in teams from hospitals with a PICU (PRE scenarios: PICU 20% vs. NON-PICU 36%; POST scenarios: PICU 79%, NON-PICU 22%; p < 0.01).
Conclusions: Our data suggest an association between airway management complexity and basic life support measures. Although the frequency of ETI was not significantly reduced after a 2-day SBT intervention, the duration of advanced airway management was shortened thus reducing no-ventilation time which led to fewer interruptions in chest compressions during simulated paediatric resuscitations. SBT may be adapted to the participants' workplace to maximize its effect and improve the overall performance in paediatric resuscitation.
Keywords: Airway management; Chest compressions; Paediatric resuscitation; Simulation training.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethical approval was obtained from the Ethics Committee of the Philipps-University of Marburg (AZ: 172/16). Written informed consent was obtained from all study participants. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Eich C, Landsleitner B. Resuscitation - cardiopulmonary resuscitation in infants and children (paediatric life support). Anasthesiol Intensivmed Notfallmed Schmerzther. 2016;51(3):196–207. - PubMed
LinkOut - more resources
Full Text Sources
