

Comparison of hypothermic and normothermic targeted temperature management in out-of-hospital cardiac arrest patients with acute coronary syndrome: a nationwide retrospective study
- PMID: 39762968
- PMCID: PMC11702027
- DOI: 10.1186/s13054-024-05235-0
Comparison of hypothermic and normothermic targeted temperature management in out-of-hospital cardiac arrest patients with acute coronary syndrome: a nationwide retrospective study
Abstract
Background: Targeted temperature management (TTM) is considered a beneficial treatment for improving outcomes in patients with OHCA due to acute coronary syndrome (ACS). The comparative benefits of hypothermic TTM (32-34°C) versus normothermic TTM (35-36°C) are unclear. This study compares these TTM strategies in improving neurological outcomes and survival rates in OHCA patients with ACS.
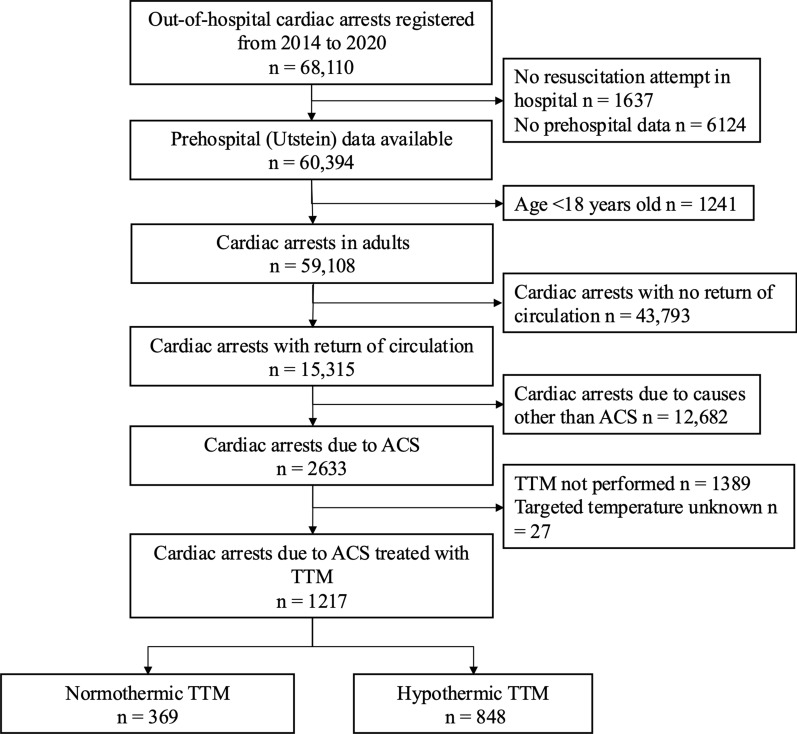
Methods: We conducted a retrospective analysis using data from the Japanese Association for Acute Medicine Out-of-Hospital Cardiac Arrest (JAAM-OHCA) registry, encompassing 68,110 OHCA patients between June 2014 and December 2020. After applying inclusion and exclusion criteria, 1,217 adult patients with ACS who received TTM were eligible for the study. Patients were categorized into two groups based on their TTM strategy: hypothermic TTM (32-34°C) and normothermic TTM (35-36°C). The primary outcome was 30-day favorable neurological outcome, defined by the Cerebral Performance Category (CPC) scale (CPC 1-2). Secondary outcomes included 30-day survival and adverse event incidence. Statistical analysis involved multivariable logistic regression and propensity score adjustments with inverse probability weighting (IPW) to account for potential confounders.
Results: Of the 1,217 patients, 369 received normothermic TTM and 848 received hypothermic TTM. In both groups, most patients were male, with a median age in the 60s. Approximately 70% had a shockable rhythm at the scene, one-third had a shockable rhythm in-hospital, around 70% had ST segment elevation, and about half received extracorporeal membrane oxygenation. The proportions of patients with 30-day favorable neurological outcomes were 36.6% (135) in the normothermic group and 36.6% (310) in the hypothermic group. No difference in neurological outcomes was observed in the multivariable regression analysis (adjusted OR 1.14, 95% CI 0.84-1.54), and the result was consistent in the IPW analysis (OR 1.11, 95% CI 0.84-1.47). Other outcomes also showed no significant differences.
Conclusion: In this nationwide, retrospective study using the JAAM-OHCA registry, we found no significant differences in 30-day favorable neurological outcome, 30-day survival, and adverse event incidences between hypothermic TTM (32-34°C) and normothermic TTM (35-36°C) in adult patients with OHCA due to ACS.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Ethics Committee of each institution approved this study protocol. Because of the observational study and de-identification of personal data, each committee waived the need for informed consent. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Luna A, Guindo J. Sudden death in ischemic heart disease. Rev Esp Cardiol. 1990;43(2):80–5.
-
- Merchant RM, Topjian AA, Panchal AR, Cheng A, Aziz K, Berg KM, et al. Part 1: executive summary: 2020 American Heart Association Guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;5:142. - PubMed
-
- Fire and Disaster Management Agency. Report on a study on social system development to improve survival from emergency cardiovascular disease (in Japanese). https://www.fdma.go.jp/publication/#rescue. Accessed June 1, 2024.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
