

Diagnostic challenges of long COVID in children: a survey of pediatric health care providers' preferences and practices
- PMID: 39764158
- PMCID: PMC11700732
- DOI: 10.3389/fped.2024.1484941
Diagnostic challenges of long COVID in children: a survey of pediatric health care providers' preferences and practices
Abstract
Introduction: Given the challenges in diagnosing children with long COVID, we sought to explore diagnostic practices and preferences among clinicians.
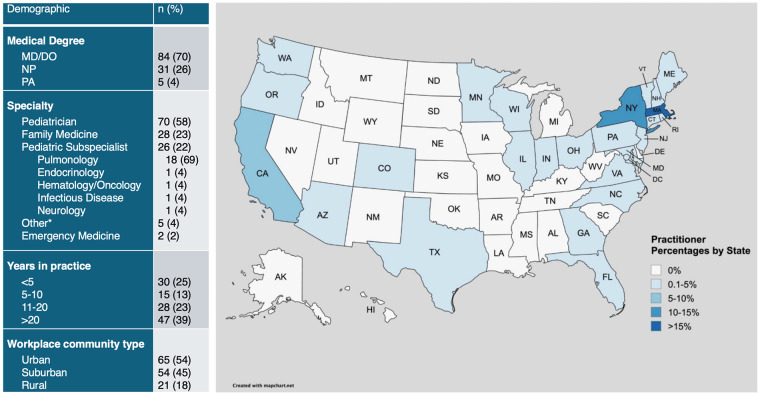
Methods: A ten-question survey assessed pediatric providers' clinical decision making for identifying and evaluating long COVID in children. Of the 120 survey respondents, 84 (70%) were physicians, 31 (26%) nurse practitioners, and 5 (4%) physician assistants.
Results: The most common categories of symptoms identified as raising suspicion for long COVID in children included cardiopulmonary symptoms, selected by 119 (99%) of pediatric providers, and neurocognitive symptoms, selected by 118 (98%) of providers. However, there was more ambiguity on the primary feature of long COVID, with providers selecting a range of key symptoms. Of all physical exam findings, postural orthostatic tachycardia, was most suggestive of long COVID [identified by 49 (41%) of pediatric providers], whereas one-third of providers reported no specific identifiable exam finding.
Discussion: Pediatric providers report variable decision making in the clinical evaluation of long COVID, with patient demographics and clinical factors impacting whether a diagnosis of long COVID is considered. This variation in diagnosing pediatric long COVID reflects ambiguity in the definition of long COVID in children and the absence of clinical guidelines to support providers in the identification of disease and treatment. This study highlights an area of need for future clinical advances in pediatric long COVID.
Keywords: COVID-19; PASC; SARS-CoV-2; long COVID; pediatric; post-acute sequalae of COVID; post-viral illness.
© 2024 Liu, Godfrey, Dunn, Fowler, Guthrie, Dredge, Holmes, Johnston, Simoneau, Fasano, Ericson and Yonker.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
-
- Center for Disease Control and Prevention, Clinical Overview of Long COVID (2024). Available online at: https://www.cdc.gov/covid/hcp/clinical-overview/index.html (Accessed August 22, 2024).
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous