

Multiple burr hole and erythropoietin combination therapy: optimal early surgical intervention for patients with acute stroke episode of moyamoya disease or moyamoya syndrome
- PMID: 39764293
- PMCID: PMC11700813
- DOI: 10.3389/fneur.2024.1479379
Multiple burr hole and erythropoietin combination therapy: optimal early surgical intervention for patients with acute stroke episode of moyamoya disease or moyamoya syndrome
Abstract
Objective: The optimal timing of bypass surgery for patients with moyamoya disease (MMD) or moyamoya syndrome (MMS) following an acute stroke episode remains unclear, mainly owing to the risk of postoperative complications. In this study, we aim to validate the safety and efficacy of early intervention using multiple burr hole (MBH) and erythropoietin (EPO) therapy, thereby refining the management strategy for patients with acute stroke episode of MMD or MMS.
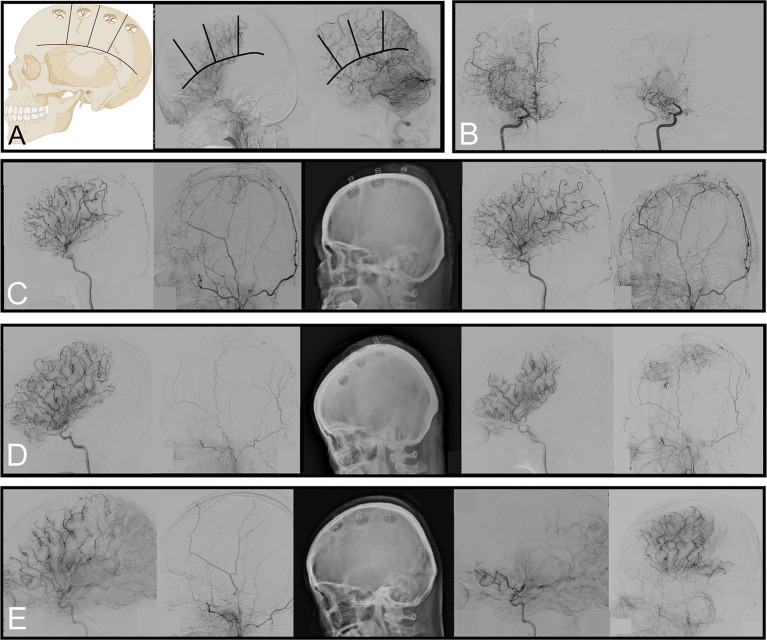
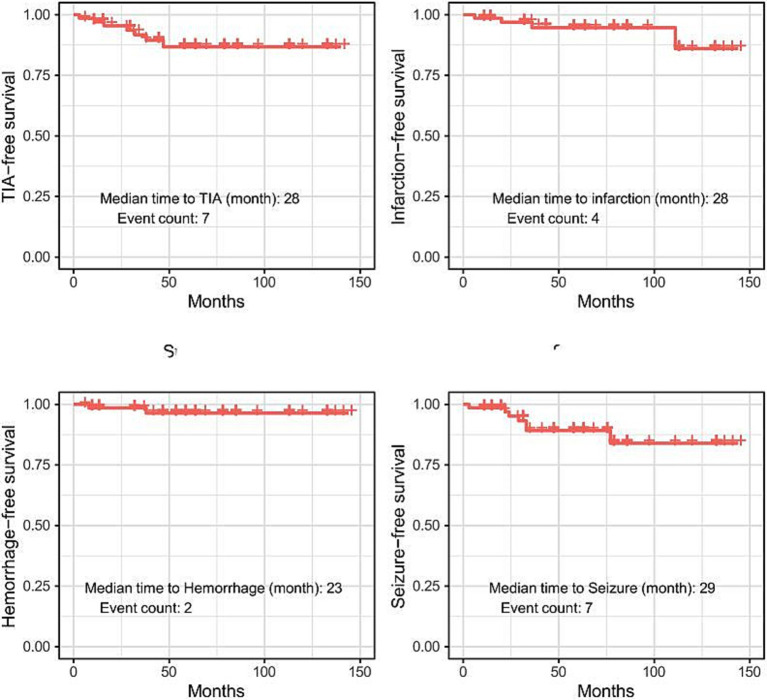
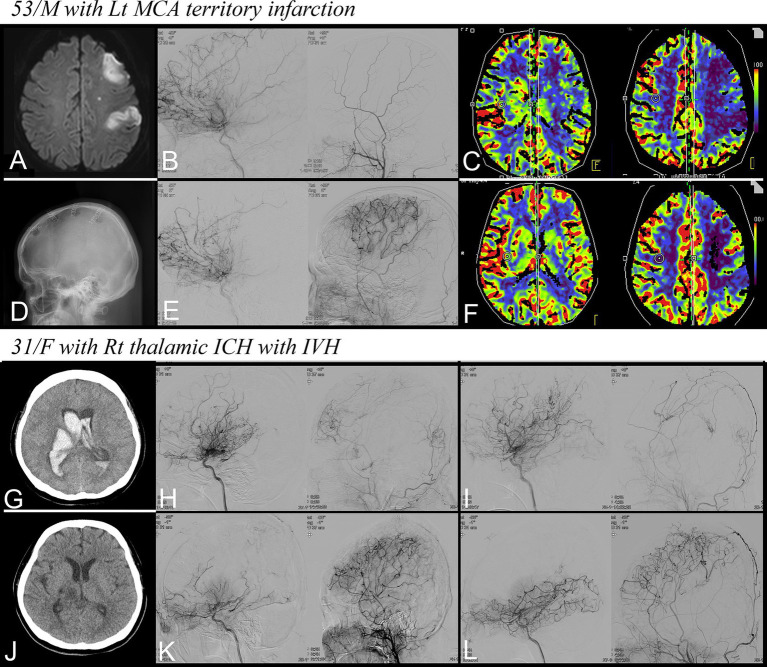
Methods: We retrospectively analyzed data from 70 patients with MMD or MMS who underwent MBH and EPO therapy. The cohort was divided based on the time interval between the latest neurological deterioration and surgery: early (<30 days) and later (≥30 days) groups. We evaluated and compared perioperative clinical parameters and the extent of neovascularization on a 6-month postoperative angiography. Long-term clinical outcomes, including transient ischemic attack (TIA), infarction, hemorrhage, and seizure, were also analyzed during the follow-up period.
Results: In the cohort, 36 patients (51.4%) were in the early group, whereas 34 (48.6%) were in the later group. The 6-month follow-up angiography demonstrated that 34/47 hemispheres (72.3%) in the early group exhibited successful neovascularization (≥2/3 of MCA territories) compared with the 19/44 (43.2%) hemispheres in the later group (odds ratio [OR] = 3.44; 95% confidence interval [CI]: 1.46-8.45; p < 0.01). In addition, a notable reduction (≥50%) in basal moyamoya vessels was observed in 30/47 hemispheres (63.8%) from the early group vs. 12/44 (27.3%) hemispheres from the later group (OR = 4.71; 95% CI: 1.97-11.82; p < 0.001). During the average follow-up of 56.5 months, only six patients experienced infarction or hemorrhage.
Conclusion: Our dataset suggests that MBH and EPO combination therapy is an effective, minimally invasive, and acceptable treatment, even in the early period of patients with MMD or MMS following an acute stroke episode.
Keywords: erythropoietin; moyamoya disease; moyamoya syndrome; multiple burr hole; surgical intervention.
Copyright © 2024 Lee, Lee, Lee, Hong and Lim.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials