

A preliminary clinical study related to vestibular migraine and cognitive dysfunction
- PMID: 39764359
- PMCID: PMC11701067
- DOI: 10.3389/fnhum.2024.1512291
A preliminary clinical study related to vestibular migraine and cognitive dysfunction
Abstract
Background and purpose: Vestibular migraine (VM) is a common clinical disorder with a genetic predisposition characterized by recurrent episodes of dizziness/vertigo. Patients often complain of the presence of cognitive dysfunction manifestations such as memory loss, which causes great distress in daily life. In this study, we will explore the characteristics and possible risk factors of VM-related cognitive dysfunction by observing the cognitive function and vestibular function status of VM patients, laying the foundation for further exploration of the mechanisms of VM-related cognitive dysfunction.
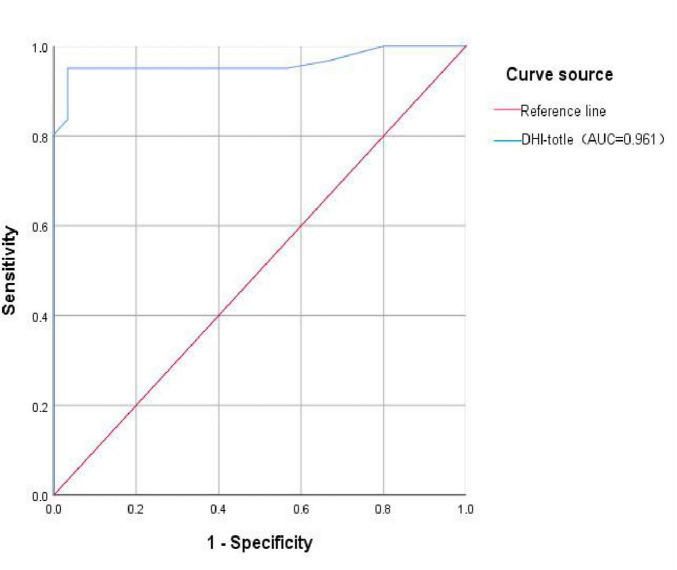
Methods: This study included 61 patients with VM and 30 healthy individuals matched for age, gender, and education level. All subjects underwent the Addenbrooke's Cognitive Examination-Revised (ACE-R), Dizziness Handicap Inventory (DHI), Hospital Anxiety and Depression Scale (HADS), Patient Health Questionnaire-9 (PHQ-9), and Generalized Anxiety Disorder-7 (GAD-7) at the first time of enrollment. Based on the ACE-R scores, the VM group was divided into the VM with cognitive dysfunction (VM-CogD) group (ACE-R < 86) and the VM without cognitive dysfunction (VM-NoCogD) group (ACE-R ≥ 86). The VM-CogD group was further categorized based on DHI scores into mild, moderate, and severe dizziness/vertigo subgroups (DHI ≤ 30 for mild, 30 < DHI ≤ 60 as moderate, and DHI > 60 as severe). All subjects underwent the head-shaking test, head-impulse test, test of skew, Romberg test, Unterberger test, videonystagmography, and caloric test to evaluate their vestibular function including the semicircular canals, vestibulo-ocular reflex pathway, and vestibulo-spinal reflex pathway. Differential analysis, correlation analysis, and ROC curve analysis were used to analyze the characteristics and influencing factors of the above clinical indicators in VM patients. It was considered that p-value < 0.05 was statistically significant, and | r| > 0.3 indicated a good correlation.
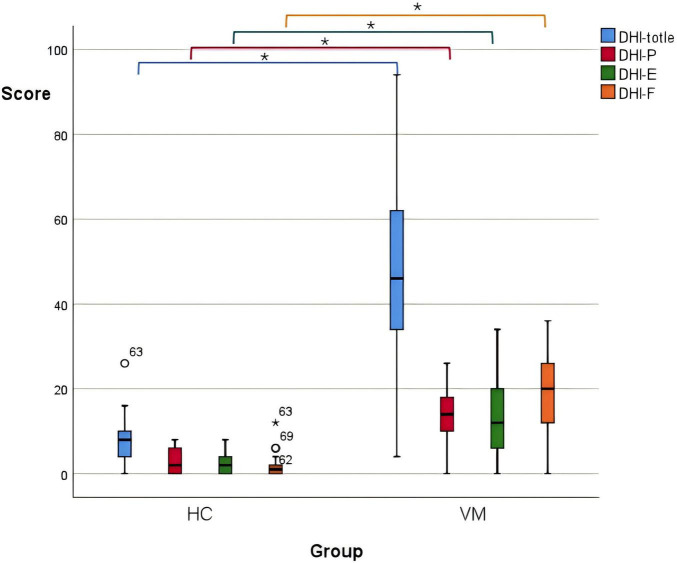
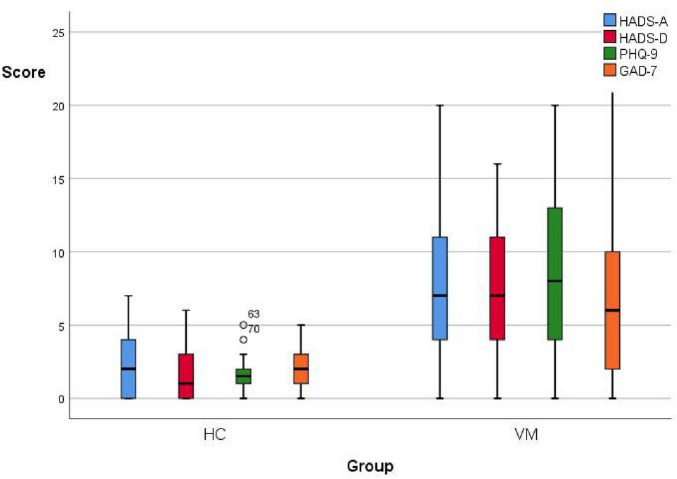
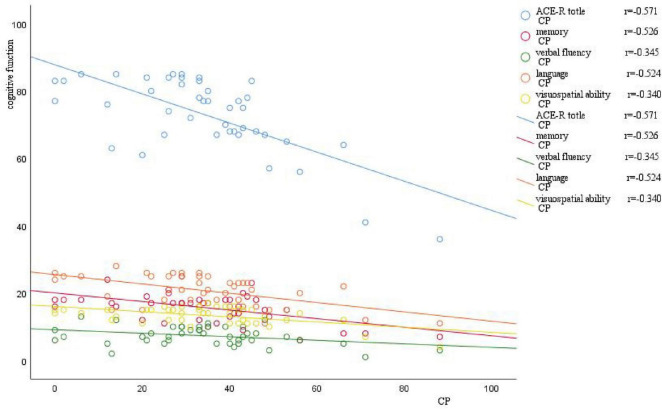
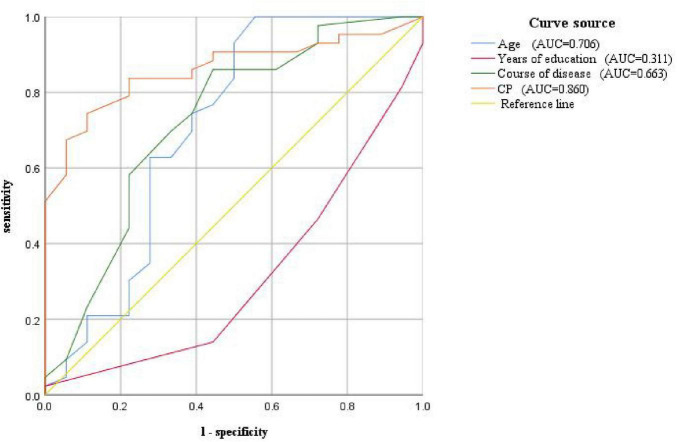
Results: There were no significant differences between the VM group and healthy control (HC) group in sex, age and education level. The total ACE-R score of the VM group was [82 (68.5, 87)], and the total ACE-R score, memory, verbal fluency, language, and visuospatial function scores were significantly lower than those of the HC group (p-value < 0.05) The percentage of horizontal semicircular canal dysfunction in the VM group (82.0%), the percentage the ocular motor dysfunction (49.2%), the positive percentage of the head-shaking test (27.9%), head-impulse test (37.7%), Romberg's sign (60.7%), and Unterberger's sign (60.7%) were significantly higher than those in the HC group (p-value < 0.05). Comparing the VM-CogD group (ACE-R < 86) with the VM-NoCogD group (ACE-R ≥ 86), the differences in Canal Paresis (CP) value, age, years of education, and duration of the disease were statistically significant (p-value < 0.05). In the VM-CogD group, CP value was negatively correlated with the ACE-R total score (r = 0.571, p-value = 0.000), memory (r = 0.526, p-value = 0.000), verbal fluency (r = 0.345, p-value = 0.024), language (r = 0.524, p-value = 0.000), and visuospatial function (r = 0.340, p-value = 0.026) scores. Age was negatively correlated with language functioning scores (r = 0.384, p-value = 0.011), and years of education was positively correlated with ACE-R total score (r = 0.504, p-value = 0.001) and language functioning (r = 0.455, p-value = 0.002) scores. When the cutoff values for the CP value, age, years of education, and duration of disease were 25.5, 33, 15.5, and 6.5, the accuracy of predicting VM-related cognitive dysfunction was the highest. The differences in DHI, DHI-P, DHI-E, DHI-F, HADS, PHQ-9, and GAD-7 scores were statistically significant between the VM group and the HC group (p-value < 0.05). In VM-CogD patients presenting with moderate dizziness/vertigo, the DHI total score was negatively correlated with the ACE-R total score (r = 0.539, p-value = 0.008), the DHI-F score was negatively correlated with the language (r = 0.450, p-value = 0.031) and visuospatial functioning part (r = 0.415, p-value = 0.049) scores, and the HADS-D scores were negatively correlated with the ACE-R total score and the part of memory functioning score (r = 0.539, p-value = 0.008).
Conclusion: (1) VM Patients exhibit multifaceted vestibular dysfunction and varying degrees of cognitive dysfunction, and cognitive function is affected by age, duration of illness, years of education, and vestibular function; (2) VM is a functional disorder, and the function disturbance, in conjunction with anxiety and depression, may participate in the occurrence of development of cognitive dysfunction in VM.
Keywords: anxiety and depression; canal paresis (CP) values; cognitive dysfunction; vestibular function; vestibular migraine.
Copyright © 2024 Sun, Lin, Huang and Pan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous