

Disparities in Surgical Intervention in Pediatric Patients With Submucous Cleft Palate and Velopharyngeal Dysfunction
- PMID: 39764682
- PMCID: PMC11947851
- DOI: 10.1002/ohn.1111
Disparities in Surgical Intervention in Pediatric Patients With Submucous Cleft Palate and Velopharyngeal Dysfunction
Abstract
Objective: To evaluate factors impacting access to and timing of surgery in patients with submucous cleft palate (SMCP) and velopharyngeal dysfunction (VPD).
Study design: Retrospective cohort study.
Setting: Single academic medical center.
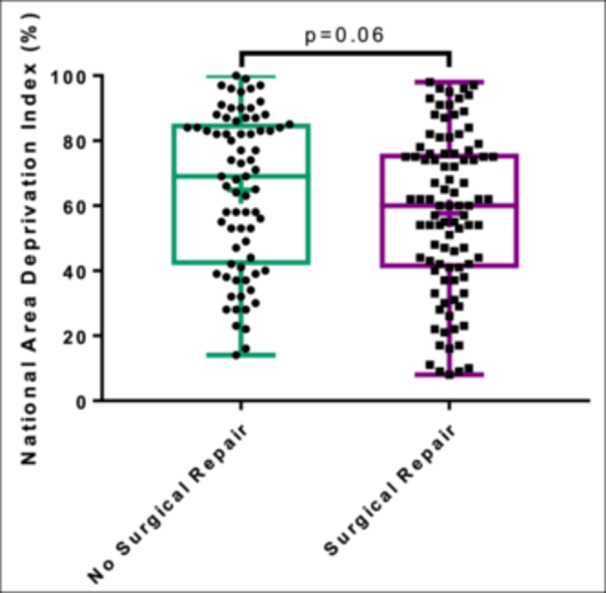
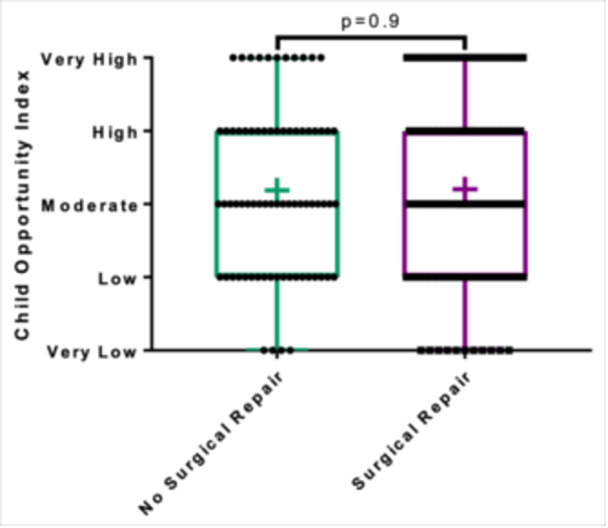
Methods: Patients with SMCP and VPD between 2004 and 2021 were identified. Variables included national and state area deprivation index (ADI) percentiles, child opportunity index (COI) categories, distance to care, and insurance status. χ2, Fisher's exact test, Wilcoxon rank-sum, Spearman rank correlation, t test, and linear regression (α = .05) were used to investigate the relationships between these variables and surgical status and timing.
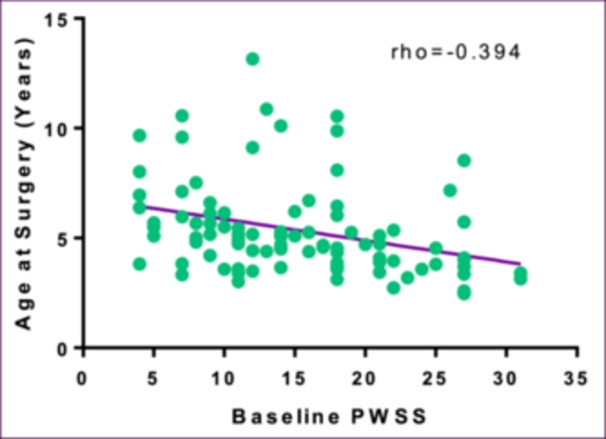
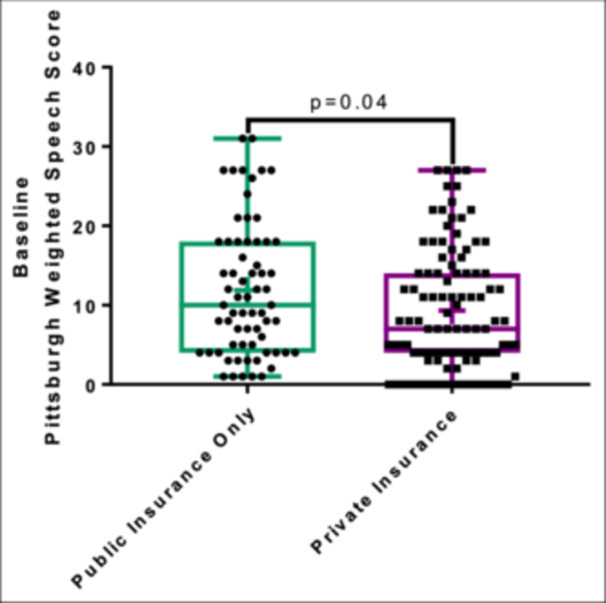
Results: A total of 168 patients were included, 94 surgical and 74 nonsurgical. Patients were predominantly white (160/168; 95.2%), Male (103/168; 61.3%), and non-Hispanic (153/168; 91.1%). There were no intergroup differences with respect to ADI, COI, insurance status, or distance from the hospital. Surgical patients were more likely to have overt SMCP (P = .03), earlier age at SMCP diagnosis (P = .02), and higher baseline Pittsburgh weighted speech score (PWSS) (P = <.001). In multivariable regression, younger age at surgery was found to be significantly associated with higher baseline PWSS (P = .001) and lower state ADI deciles (P = .03). Patients with private insurance had a lower baseline PWSS than those with public insurance (P = .04). Insurance status was not significantly associated with age at diagnosis (P = .79) or age at surgery (P = .08).
Conclusion: In this study, patients from less disadvantaged neighborhoods were found to have earlier surgical intervention, highlighting the importance of incorporating social determinants of health in the evaluation of VPD and SMCP patients to prevent treatment delays.
Keywords: area deprivation index; child opportunity index; disparities; submucous cleft palate; velopharyngeal dysfunction.
© 2025 The Author(s). Otolaryngology–Head and Neck Surgery published by Wiley Periodicals LLC on behalf of American Academy of Otolaryngology–Head and Neck Surgery Foundation.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Michael AI, Olorunfemi G, Olusanya A, Oluwatosin O. Trends of cleft surgeries and predictors of late primary surgery among children with cleft lip and palate at the University College Hospital, Nigeria: A retrospective cohort study. PLoS One. 2023;18(1):e0274657. 10.1371/journal.pone.0274657 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
