

Revisiting Antibiotic-Impregnated Cement Spacer for Diabetic Osteomyelitis of the Foot
- PMID: 39766543
- PMCID: PMC11672849
- DOI: 10.3390/antibiotics13121153
Revisiting Antibiotic-Impregnated Cement Spacer for Diabetic Osteomyelitis of the Foot
Abstract
Introduction: Despite the rising global awareness and improvement of socioeconomic and living standards, the prevalence of diabetic osteomyelitis (DOM) and its complications has been increasing rapidly. This study aims to investigate the long-term prognosis of DOM of the foot treated using antibiotic-impregnated cement spacer (ACS) and the contributing risk factors for reoperation.
Methods and materials: We retrospectively reviewed the data of 55 diabetic patients with Meggitt-Wagner Grade IIB wounds diagnosed with osteomyelitis of the foot, treated in our institution with excessive debridement, excision of the infected tissue, and implantation of antibiotic-impregnated cement spacer fixed with a Kirschner wire. Descriptive statistics, including patient demographics, were analyzed. Statistical analysis was performed using point-biserial correlation and a Chi-square test with Cramer's V effect-size estimation to determine the relationship between reoperation and various parameters.
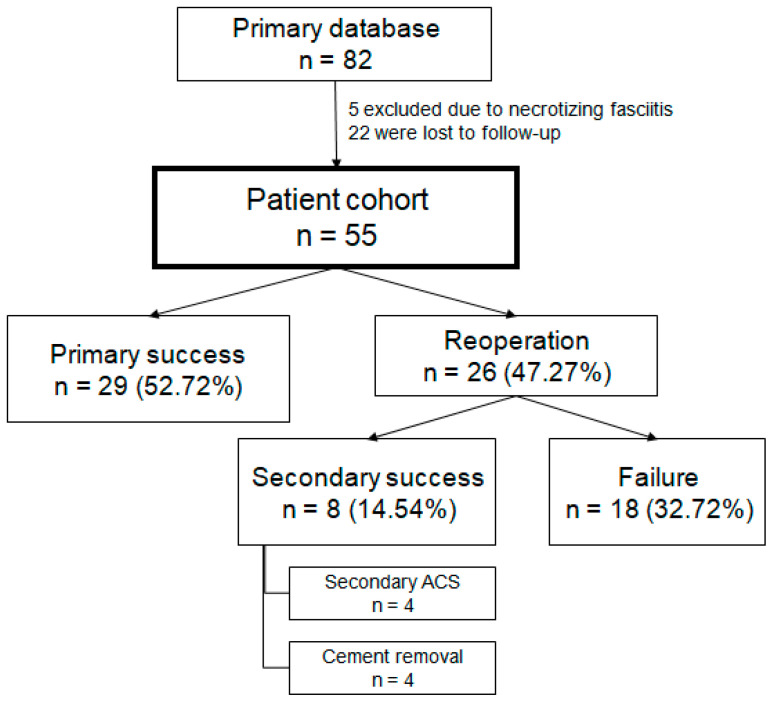
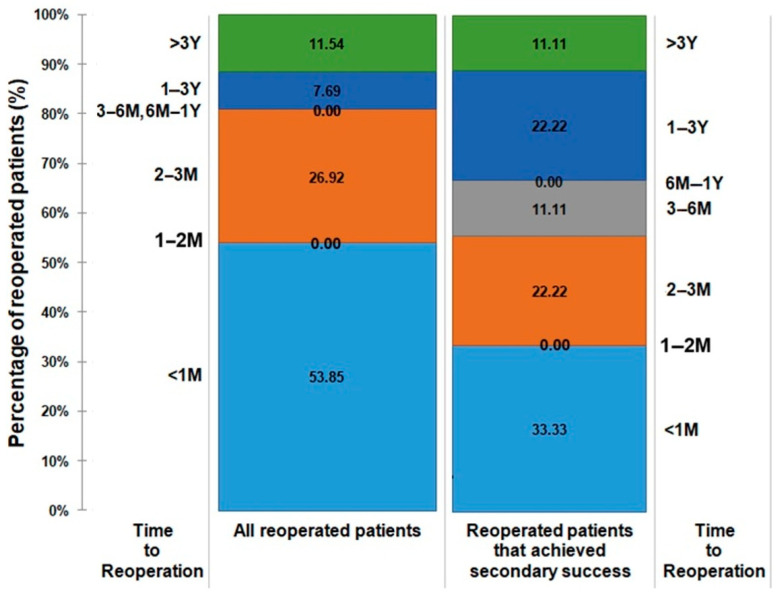
Results: 55 patients (36 (65.45%) males and 19 (34.55%) females) with a median age of 64 (39-84) years were thoroughly analyzed throughout a median follow-up of 884 days (2-4671 days). Of the entire cohort, 29 (52.72%) patients achieved primary successful infection eradication without any further intervention, and 8 (14.54%) patients were successfully treated using a secondary procedure. More than half of the reoperated patients underwent the secondary intervention within less than a month after the primary ACS. When assessing correlation, age (r = 0.28, p = 0.04), gender (r = 0.31, p = 0.02), Staphylococcus aureus (r = -0.10, p = 0.04), and the use of gentamicin-only antibiotic cement spacer (r = 0.34, p = 0.01) demonstrated statistically significant correlation to reoperation. 89.18% of the patients who achieved infection eradication did not undergo cement removal.
Conclusions: ACS has shown excellent results in eradicating bone infection with up to 7.23 years of follow-up, acting as a structural stabilizer, preventing soft tissue contractures, and delivering highly concentrated local antibiotic treatment both to soft tissue and bone. Regardless, specific factors should be thoroughly evaluated prior to surgery, as advancing age, gender, and the use of gentamicin-only antibiotics appear to be positively associated with a higher likelihood of reoperation. Conversely, infections caused by cultured Staphylococcus aureus seem to be inversely related to reoperation.
Keywords: antibiotic PMMA; antibiotic cement-spacer; diabetic foot; osteomyelitis; resection arthroplasty.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Qi X., Ge X., Chen X., Cai E., Xiang Y., Xu H., Li Y., Lan Y., Shi Y., Deng H., et al. An Immunoregulation Hydrogel with Controlled Hyperthermia-Augmented Oxygenation and ROS Scavenging for Treating Diabetic Foot Ulcers. Adv. Funct. Mater. 2024;34:2400489. doi: 10.1002/adfm.202400489. - DOI
LinkOut - more resources
Full Text Sources
