

Prescriptive Appropriateness and Efficacy of Cholesterol-Lowering Drugs in a Secondary Prevention Setting-A Retrospective Analysis from Two Italian Cardiac Rehabilitation Centers
- PMID: 39768428
- PMCID: PMC11677457
- DOI: 10.3390/jcm13247505
Prescriptive Appropriateness and Efficacy of Cholesterol-Lowering Drugs in a Secondary Prevention Setting-A Retrospective Analysis from Two Italian Cardiac Rehabilitation Centers
Abstract
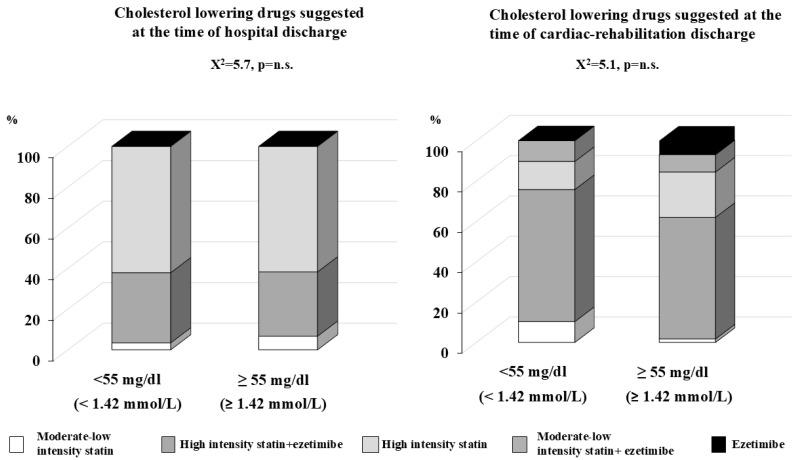
Background: Treatment of CV risk factors, such as cholesterol level, represents one of the main goals to reduce atherosclerotic burden. The aim of this study was to investigate the prescriptive appropriateness of cholesterol-lowering drugs among patients who experienced an atherosclerotic CV disease (ASCVD). Methods: We investigated 155 patients who underwent cardiac rehabilitation in 2020. The European Society of Cardiology (ESC) 2021 guidelines on CV disease prevention and 2019 ESC Guidelines on dyslipidemias were followed to detect the appropriateness of prescription. SCORE2 and SCORE2-OP risk estimations were used to detect patients' CV risk profiles. Patients were divided into three groups: 1 (n = 118) patients admitted for their first CV event, 2A (n = 18) patients who experienced a previous CV event years before, and 2B (n = 19) patients admitted for a new event with a previous CV event 2 years before. Low-density lipoprotein (LDL) cholesterol level was detected at the time of admission to the hospital, during cardiac rehabilitation, and at the first visit after rehabilitation. Results: The statistics for our study participants, with a mean age of 66.1 years, were: 72.4% overweight/obese, 63.9% diabetic, 72.5% smokers, 93.0% hypertensives, and 91.7% had dyslipidemias. In group 1, only 5.1% had a low/moderate risk, 44.1% presented a high risk, and 50.8% a very high risk according to calculators. The average LDL levels were 115.8 mg/dL (2.99 mol/L) upon admission to the hospital, 66.4 mg/dL (1.72 mmol/L) at the time of cardiac rehabilitation, and 64.8 mg/dL (1.67 mmol/L) at the subsequent medical visit. In the overall group, only 36.0% had LDL < 55 mg/dL (1.42 mmol/L). In group 1, 79.4% were treated with high-intensity statin alone or plus ezetimibe; in group 2A, the percentage increased up to 87.5%, while group 2B 33.4% was treated with high-intensity statin plus ezetimibe and 33.3% were treated with PCSK9 inhibitors. Conclusions: This retrospective study confirms the importance of properly calculating CV risk profiles. The main limitations for the efficacy of lipid-lowering drugs were: patient's compliance, drugs side effects, lifestyle habits, and collaboration with a general practitioner.
Keywords: adherence to treatment; cardiac rehabilitation; cardiovascular disease; dyslipidemias; statin.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



References
-
- Roth G.A., Abate D., Abate K.H. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1736–1788. doi: 10.1016/S0140-6736(18)32203-7. - DOI - PMC - PubMed
-
- Mach F., Baigent C., Catapano A.L., Koskinas K.C., Casula M., Badimon L., Chapman M.J., De Backer G.G., Delgado V., Ference B.A., et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020;41:111–188. doi: 10.1093/eurheartj/ehz455. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
