

Mechanistic Relevance of Ventricular Arrhythmias in Heart Failure with Preserved Ejection Fraction
- PMID: 39769189
- PMCID: PMC11677834
- DOI: 10.3390/ijms252413423
Mechanistic Relevance of Ventricular Arrhythmias in Heart Failure with Preserved Ejection Fraction
Abstract
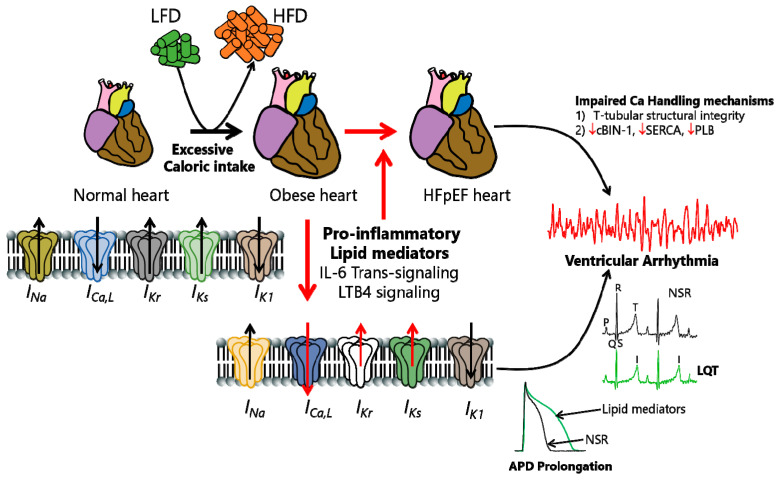
Heart failure with preserved ejection fraction (HFpEF) is increasing at an alarming rate worldwide, with limited effective therapeutic interventions in patients. Sudden cardiac death (SCD) and ventricular arrhythmias present substantial risks for the prognosis of these patients. Obesity is a risk factor for HFpEF and life-threatening arrhythmias. Obesity and its associated metabolic dysregulation, leading to metabolic syndrome, are an epidemic that poses a significant public health problem. More than one-third of the world population is overweight or obese, leading to an enhanced risk of incidence and mortality due to cardiovascular disease (CVD). Obesity predisposes patients to atrial fibrillation and ventricular and supraventricular arrhythmias-conditions that are caused by dysfunction in the electrical activity of the heart. To date, current therapeutic options for the cardiomyopathy of obesity are limited, suggesting that there is considerable room for the development of therapeutic interventions with novel mechanisms of action that will help normalize sinus rhythms in obese patients. Emerging candidates for modulation by obesity are cardiac ion channels and Ca-handling proteins. However, the underlying molecular mechanisms of the impact of obesity on these channels and Ca-handling proteins remain incompletely understood. Obesity is marked by the accumulation of adipose tissue, which is associated with a variety of adverse adaptations, including dyslipidemia (or abnormal systemic levels of free fatty acids), increased secretion of proinflammatory cytokines, fibrosis, hyperglycemia, and insulin resistance, which cause electrical remodeling and, thus, predispose patients to arrhythmias. Furthermore, adipose tissue is also associated with the accumulation of subcutaneous and visceral fat, which is marked by distinct signaling mechanisms. Thus, there may also be functional differences in the effects of the regional distribution of fat deposits on ion channel/Ca-handling protein expression. Evaluating alterations in their functional expression in obesity will lead to progress in the knowledge of the mechanisms responsible for obesity-related arrhythmias. These advances are likely to reveal new targets for pharmacological modulation. Understanding how obesity and related mechanisms lead to cardiac electrical remodeling is likely to have a significant medical and economic impact. Nevertheless, substantial knowledge gaps remain regarding HFpEF treatment, requiring further investigations to identify potential therapeutic targets. The objective of this study is to review cardiac ion channel/Ca-handling protein remodeling in the predisposition to metabolic HFpEF and arrhythmias. This review further highlights interleukin-6 (IL-6) as a potential target, cardiac bridging integrator 1 (cBIN1) as a promising gene therapy agent, and leukotriene B4 (LTB4) as an underappreciated pathway in future HFpEF management.
Keywords: arrhythmias; diabetes; heart failure; ion channel remodeling; obesity; sudden cardiac death; ventricular.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Systemic Inflammatory Response Syndrome.2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31613449 Free Books & Documents.
-
Interventions for weight reduction in obesity to improve survival in women with endometrial cancer.Cochrane Database Syst Rev. 2023 Mar 27;3(3):CD012513. doi: 10.1002/14651858.CD012513.pub3. Cochrane Database Syst Rev. 2023. PMID: 36971688 Free PMC article.
-
Cardiac Ion Channel Regulation in Obesity and the Metabolic Syndrome: Relevance to Long QT Syndrome and Atrial Fibrillation.Front Physiol. 2017 Jun 21;8:431. doi: 10.3389/fphys.2017.00431. eCollection 2017. Front Physiol. 2017. PMID: 28680407 Free PMC article. Review.
-
Interplay of Chronic Kidney Disease and the Effects of Tirzepatide in Patients With Heart Failure, Preserved Ejection Fraction, and Obesity: The SUMMIT Trial.J Am Coll Cardiol. 2025 May 13;85(18):1721-1735. doi: 10.1016/j.jacc.2025.03.009. Epub 2025 Mar 31. J Am Coll Cardiol. 2025. PMID: 40162940 Clinical Trial.
References
-
- McDonagh T.A., Metra M., Adamo M., Gardner R.S., Baumbach A., Böhm M., Burri H., Butler J., Čelutkienė J., Chioncel O., et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021;42:3599–3726. doi: 10.1093/eurheartj/ehab368. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
