

Advancements and Challenges in the Management of Prosthetic Valve Endocarditis: A Review
- PMID: 39770299
- PMCID: PMC11728846
- DOI: 10.3390/pathogens13121039
Advancements and Challenges in the Management of Prosthetic Valve Endocarditis: A Review
Abstract
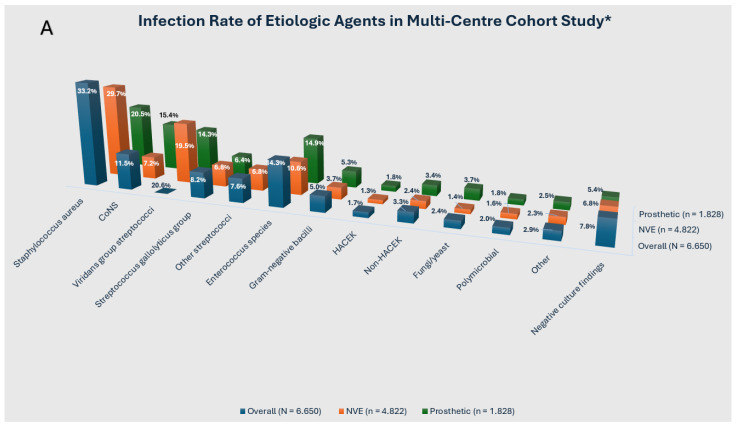
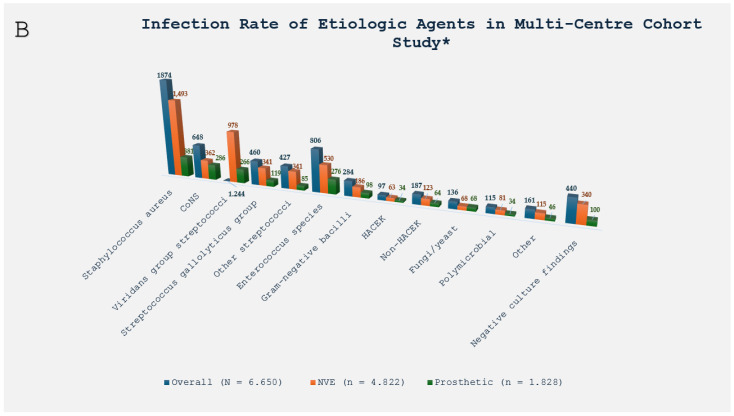
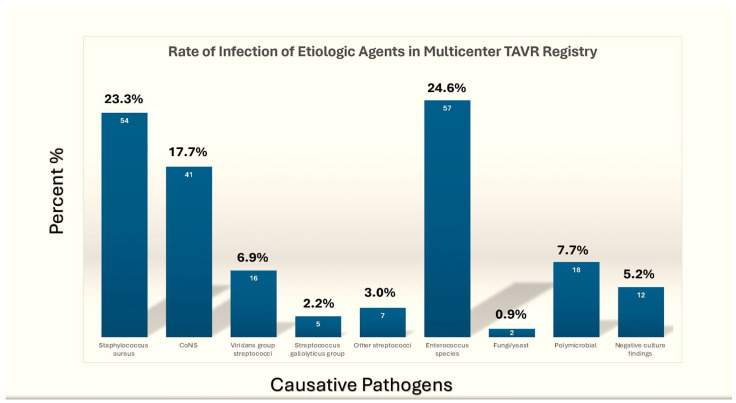
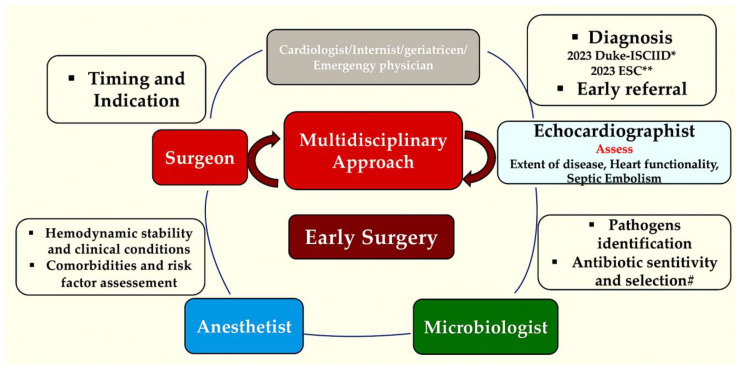
Prosthetic valve endocarditis (PVE) is the medical term used to describe a focus of infection involving a valvular substitute within the heart. It is a significant concern in the field of cardiology, and the epidemiology of PVE has seen notable developments over the last five decades. The disease currently affects an older demographic and is becoming increasingly prevalent in patients with transcatheter-implanted valves. It is imperative that we urgently address the significant challenges posed by PVE. It is a disease that has a wide range of potential aetiologies, clinical presentations, and courses. In developed countries, Staphylococcus aureus is now the predominant causative organism, resulting in an aggressive form of disease that frequently afflicts vulnerable or elderly populations. However, it is clear that Enterococcus species present a significant challenge in the context of PVE following TAVR procedures, given their elevated prevalence. The 2023 Duke/International Society for Cardiovascular Infectious Diseases infective endocarditis diagnostic criteria now include significant developments in microbiological and image-based techniques for diagnostic purposes, specifically the incorporation of fluorine-18 fluorodeoxyglucose positron emission tomography and computed tomography. These developments unequivocally enhance the diagnostic sensitivity for PVE, while maintaining the specificity. They do so in accordance with the results of studies conducted specifically for the purpose of validation. The lack of rigorous scientific studies and a shortage of funding and resources for research have led to a significant gap in our understanding. Randomized controlled trials could provide invaluable insight and guidance for clinical practice, but they are missing, which represents a major gap. It is clear that there is an urgent need for more research. PVE is a life-threatening condition that must be handled by a multidisciplinary endocarditis team at a cardiac centre in order to improve outcomes. The emergence of innovative surgical techniques has empowered clinicians to steer more patients away from surgical procedures, despite the presence of clear indications for them. A select group of patients can now complete parenteral or oral antimicrobial treatment at home. Additionally, antibiotic prophylaxis is the best option for individuals with prosthetic valves who are going to have invasive dental procedures. These individuals should be given antibiotics beforehand.
Keywords: TAVR; infective endocarditis; prosthetic valve endocarditis; vegetation.
Conflict of interest statement
The author declares no conflict of interest.
Figures

References
-
- Otto C.M., Nishimura R.A., Bonow R.O., Carabello B.A., Erwin J.P., III, Gentile F., Jneid H., Krieger E.V., Mack M., McLeod C., et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. J. Am. Coll. Cardiol. 2021;77:e25–e197. doi: 10.1016/j.jacc.2020.11.018. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
