

Association of Protein Intake with Sarcopenia and Related Indicators Among Korean Older Adults: A Systematic Review and Meta-Analysis
- PMID: 39770971
- PMCID: PMC11677379
- DOI: 10.3390/nu16244350
Association of Protein Intake with Sarcopenia and Related Indicators Among Korean Older Adults: A Systematic Review and Meta-Analysis
Abstract
Objectives: Due to variations in the standards for optimal protein intake and conflicting results across studies for Korean older adults, this study aimed to quantitatively integrate existing research on the association of protein intake with sarcopenia and related indicators in Koreans aged 65 and older through meta-analysis.
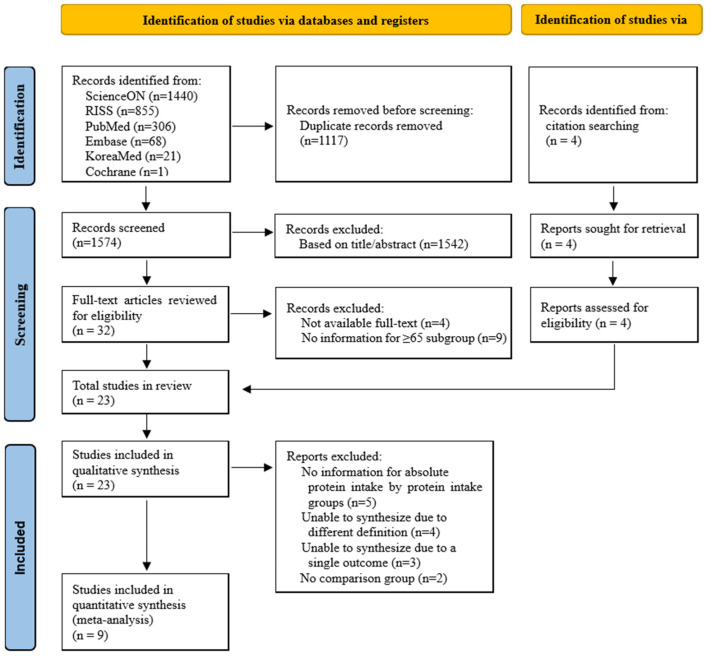
Methods: A total of 23 studies were selected according to the study selection criteria (PICOS). Sixteen cross-sectional studies, 5 randomized controlled trials (RCTs), and 2 non-RCTs were included in the review, with 9 out of 23 studies included in the meta-analysis. We used fixed-effects models and performed subgroup and sensitivity analyses.
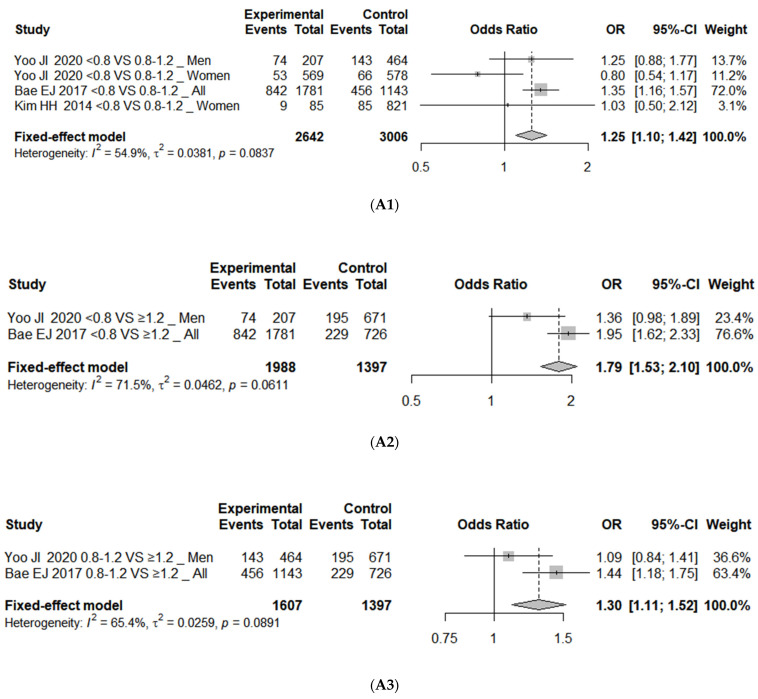
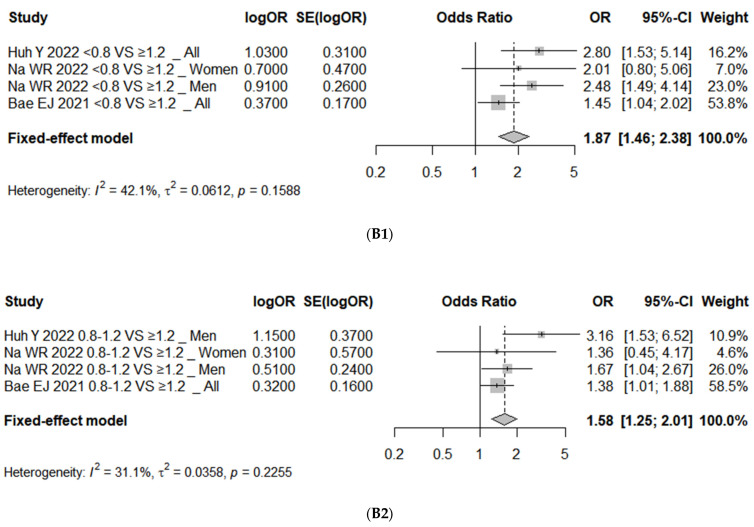
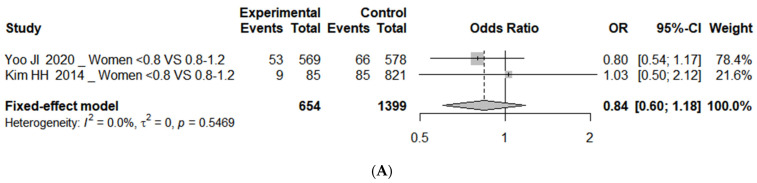
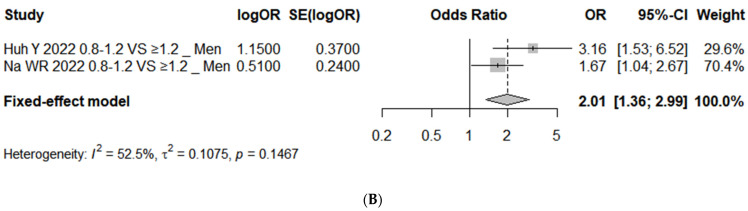
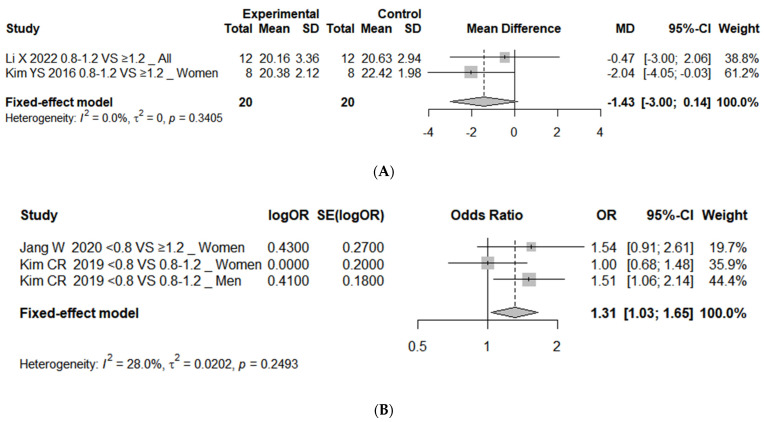
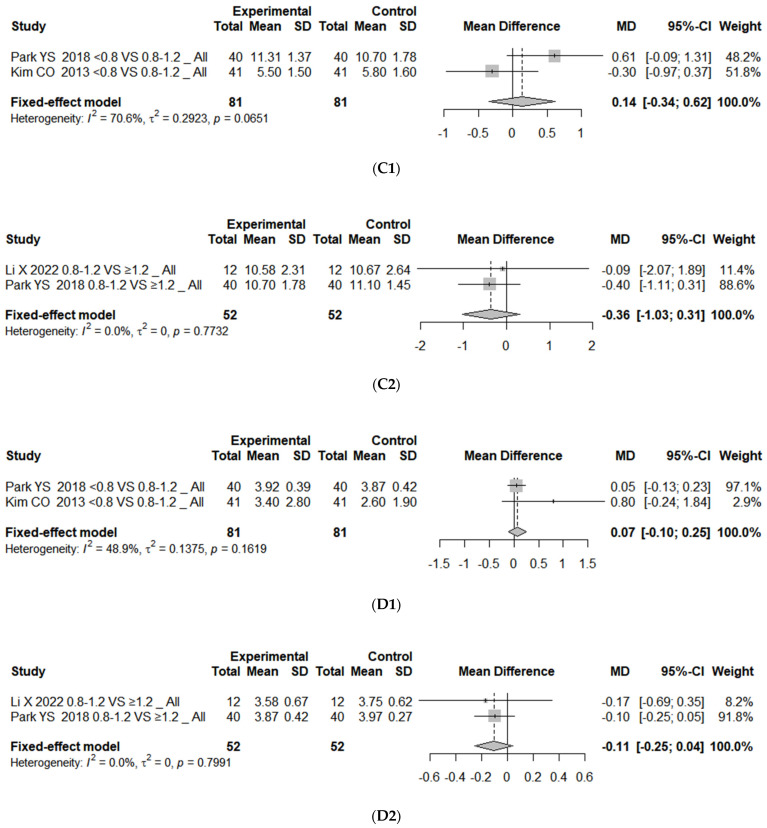
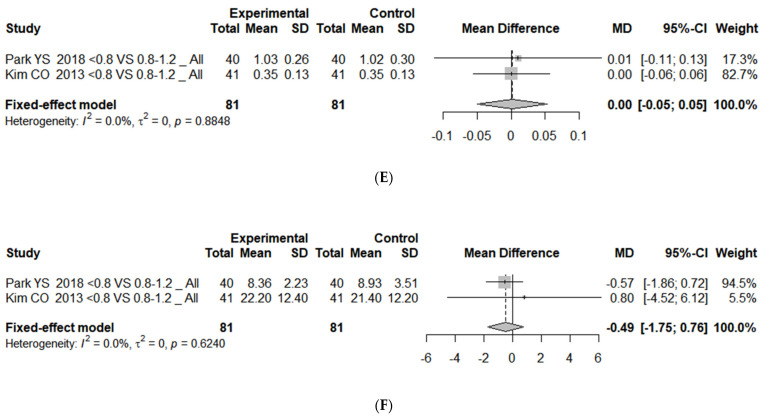
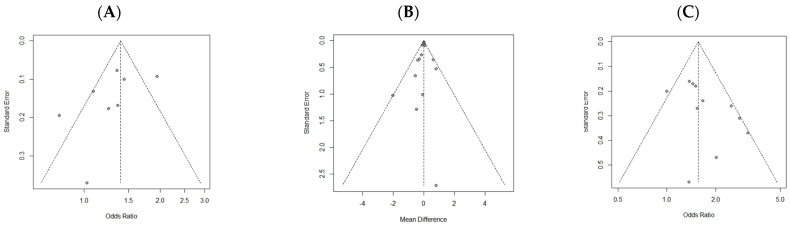
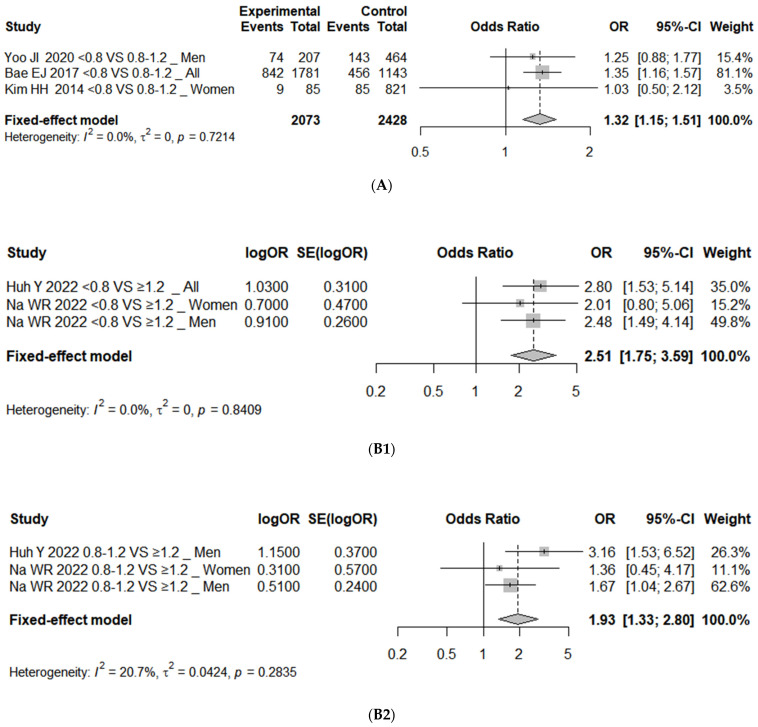
Results: A meta-analysis found that the risk of sarcopenia was significantly higher in the <0.8 g/kg/day protein intake group compared to the 0.8-1.2 g/kg/day and ≥1.2 g/kg/day groups, with odds ratios (ORs) of 1.25 (95% confidence interval (CI), 1.10 to 1.42; I2 = 55%) and 1.79 (95% CI, 1.53 to 2.10; I2 = 71%), respectively. For low hand grip strength (HGS), the risk was higher in the <0.8 g/kg/day group compared to the 0.8-1.2 g/kg/day or ≥1.2 g/kg/day groups (OR 1.31; 95% CI, 1.03 to 1.65; I2 = 28%). No significant associations were found with other sarcopenia indicators, such as skeletal muscle mass, short physical performance battery score, balance test, gait speed, and timed up-and-go test.
Conclusions: Lower protein intake is associated with a higher risk of sarcopenia and low HGS in Korean older adults. To establish protein intake recommendations for the prevention and management of sarcopenia in this population, further well-designed RCTs incorporating both protein supplementation and resistance training are necessary.
Keywords: Korean; aged; meta-analysis; protein; sarcopenia; systematic review.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
References
-
- Fielding R.A., Vellas B., Evans W.J., Bhasin S., Morley J.E., Newman A.B., Abellan van Kan G., Andrieu S., Bauer J., Breuille D., et al. Sarcopenia: An undiagnosed condition in older adults. Current consensus definition: Prevalence, etiology, and consequences. International working group on sarcopenia. J. Am. Med. Dir. Assoc. 2011;12:249–256. doi: 10.1016/j.jamda.2011.01.003. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
