

The Development of an Age-Appropriate Fixed Dose Combination for Tuberculosis Using Physiologically-Based Pharmacokinetic Modeling (PBBM) and Risk Assessment
- PMID: 39771565
- PMCID: PMC11680012
- DOI: 10.3390/pharmaceutics16121587
The Development of an Age-Appropriate Fixed Dose Combination for Tuberculosis Using Physiologically-Based Pharmacokinetic Modeling (PBBM) and Risk Assessment
Abstract
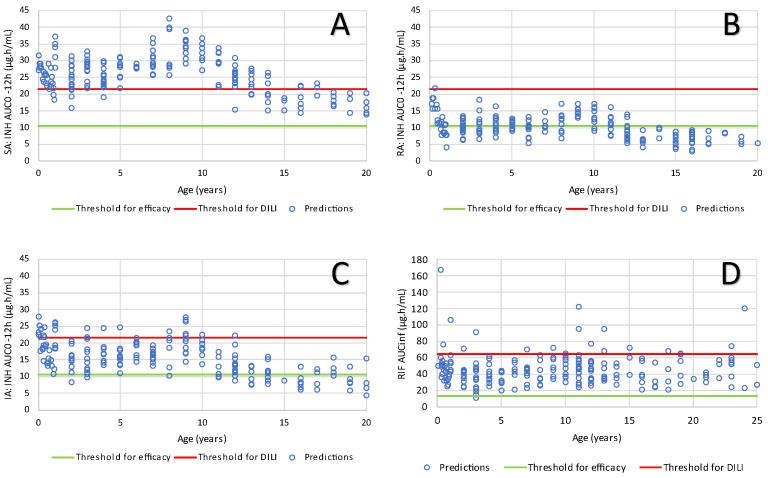
Background/Objectives: The combination of isoniazid (INH) and rifampicin (RIF) is indicated for the treatment maintenance phase of tuberculosis (TB) in adults and children. In Brazil, there is no current reference listed drug for this indication in children. Farmanguinhos has undertaken the development of an age-appropriate dispersible tablet to be taken with water for all age groups from birth to adolescence. The primary objective of this work was to develop and validate a physiologically-based biopharmaceutics model (PBBM) in GastroPlusTM, to link the product's in vitro performance to the observed pharmacokinetic (PK) data in adults and children. Methods: The PBBM was developed based on measured or predicted physico-chemical and biopharmaceutical properties of INH and RIF. The metabolic clearance was specified mechanistically in the gut and liver for both parent drugs and acetyl-isoniazid. The model incorporated formulation related measurements such as dosage form disintegration and dissolution as inputs and was validated using extensive literature as well as in house clinical data. Results: The model was used to predict the exposure in children across the targeted dosing regimen for each age group using the new age-appropriate formulation. Probabilistic models of efficacy and safety versus exposure, combined with real world data on children, were utilized to assess drug efficacy and safety in the target populations. Conclusions: The model predictions (systemic exposure) along with clinical data from the literature linking systemic exposure to clinical outcomes confirmed that the proposed dispersible pediatric tablet and dosing regimen are anticipated to be as safe and as effective as adult formulations at similar doses.
Keywords: PBBM; efficacy; formulation; modeling; pediatrics; safety; simulation; tuberculosis.
Conflict of interest statement
Xavier J.H. Pepin and Sandra Suarez-Sharp are employees of and hold stock in Simulations Plus, which was commissioned by Farmanguinhos/Fiocruz to conduct the study. The company Farmanguinhos/Fiocruz helped review the manuscript, commissioned clinical trials STPh 71/10 and STPh 08/19 (2 out of the 30 clinical trials used for model validation), the data of which was reviewed by ANVISA.
Figures






References
-
- Brouwer K.L., Aleksunes L.M., Brandys B., Giacoia G.P., Knipp G., Lukacova V., Meibohm B., Nigam S.K., Rieder M., de Wildt S.N. Human Ontogeny of Drug Transporters: Review and Recommendations of the Pediatric Transporter Working Group. Clin. Pharmacol. Ther. 2015;98:266–287. doi: 10.1002/cpt.176. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
