

Mapping the HPV Landscape in South African Women: A Systematic Review and Meta-Analysis of Viral Genotypes, Microbiota, and Immune Signals
- PMID: 39772200
- PMCID: PMC11680443
- DOI: 10.3390/v16121893
Mapping the HPV Landscape in South African Women: A Systematic Review and Meta-Analysis of Viral Genotypes, Microbiota, and Immune Signals
Abstract
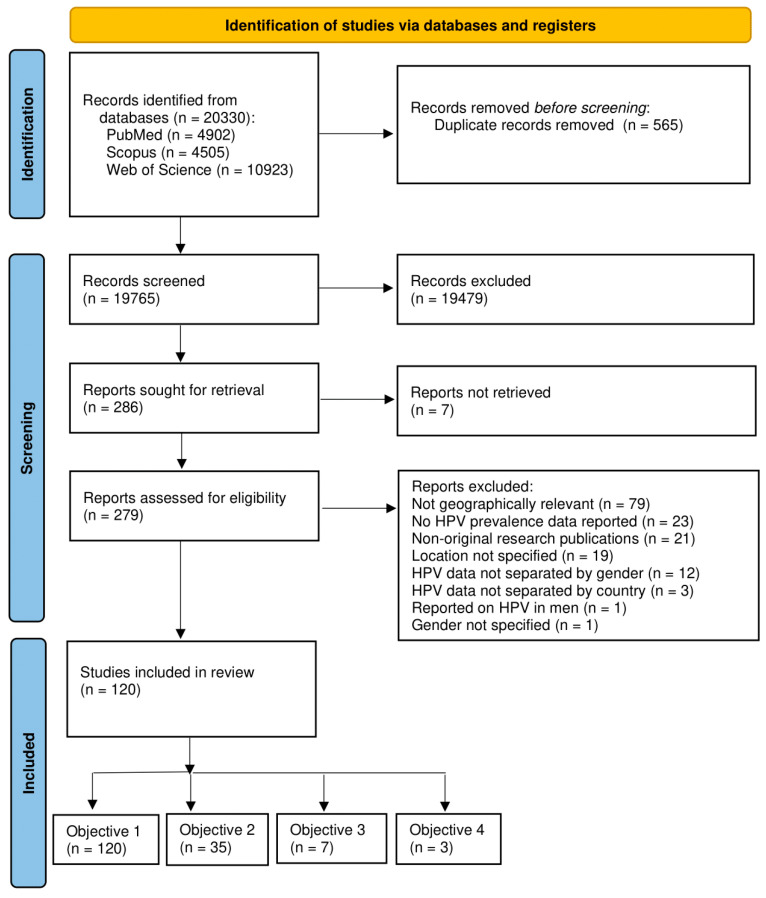
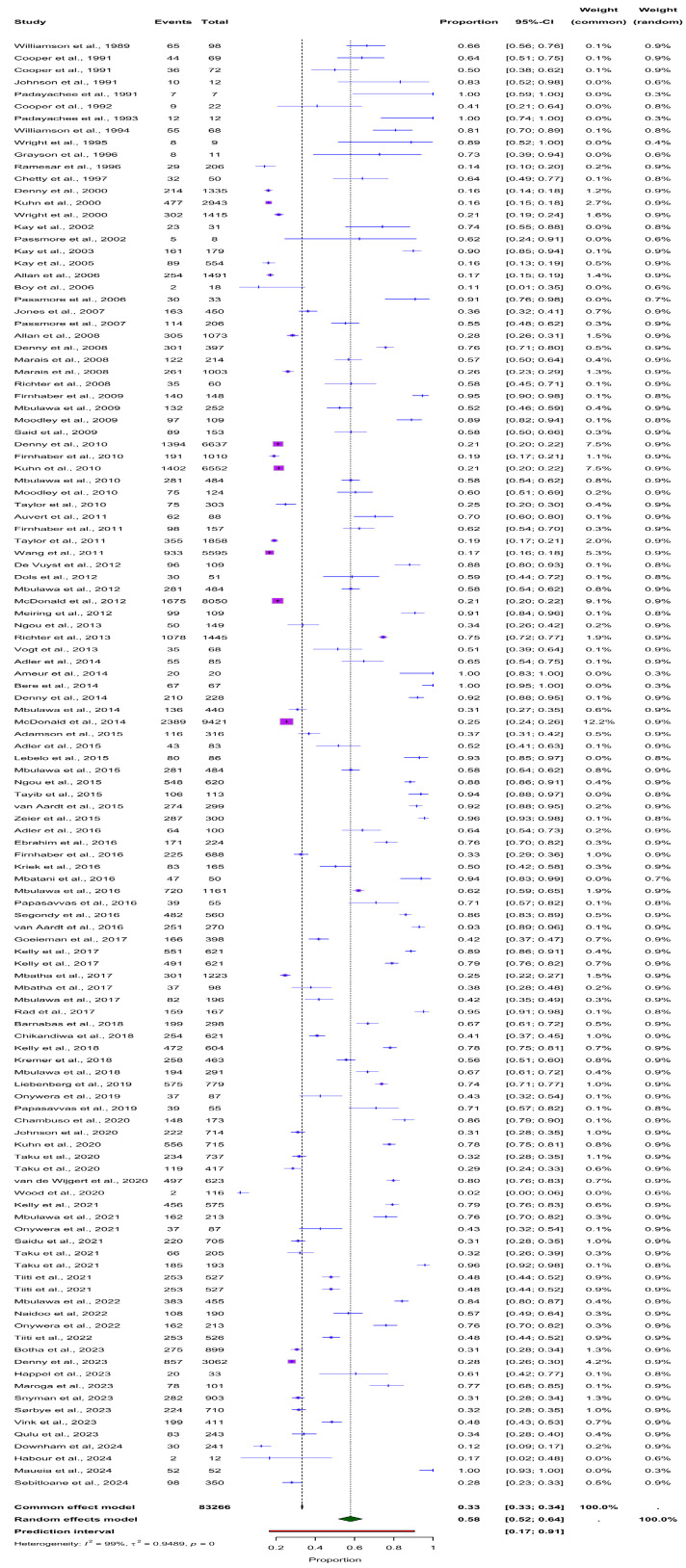
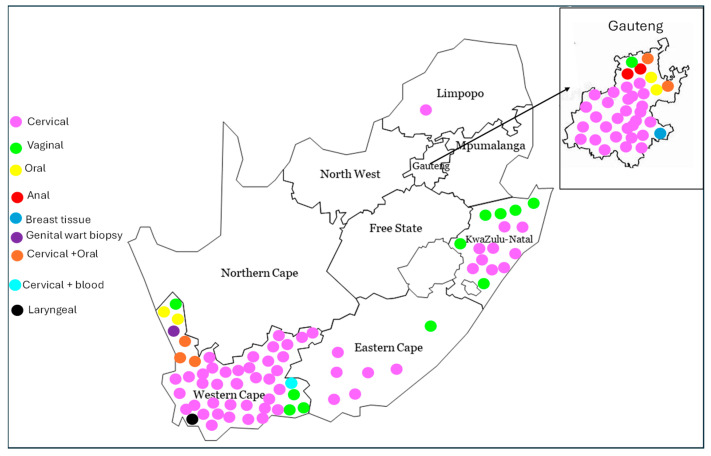
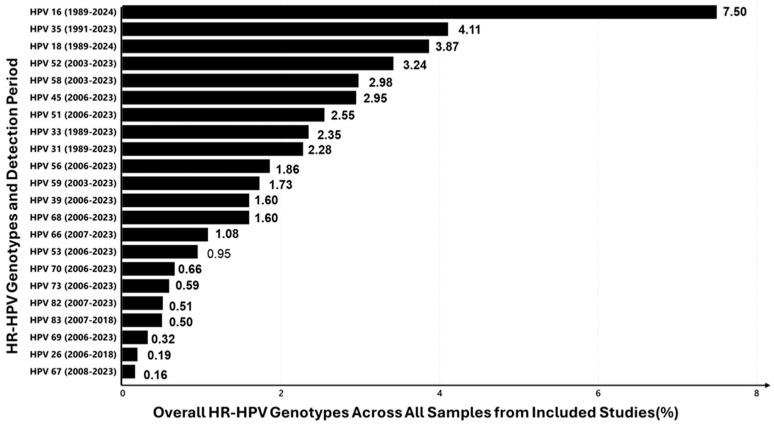
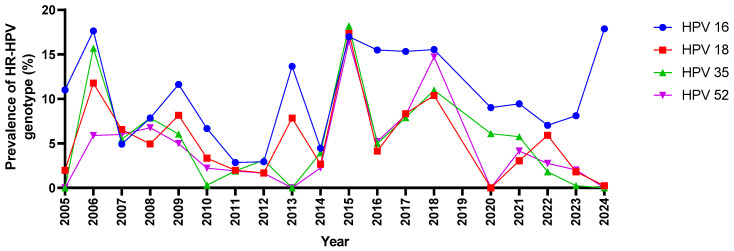
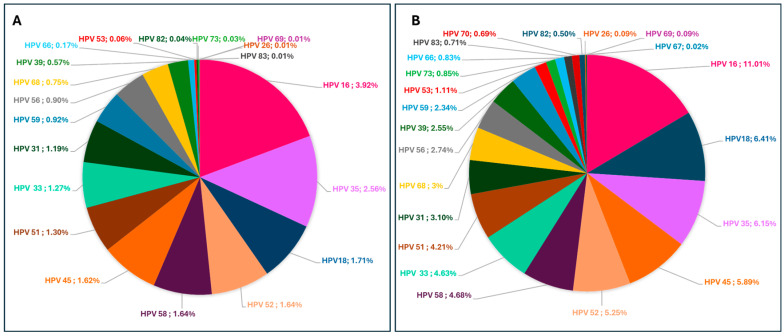
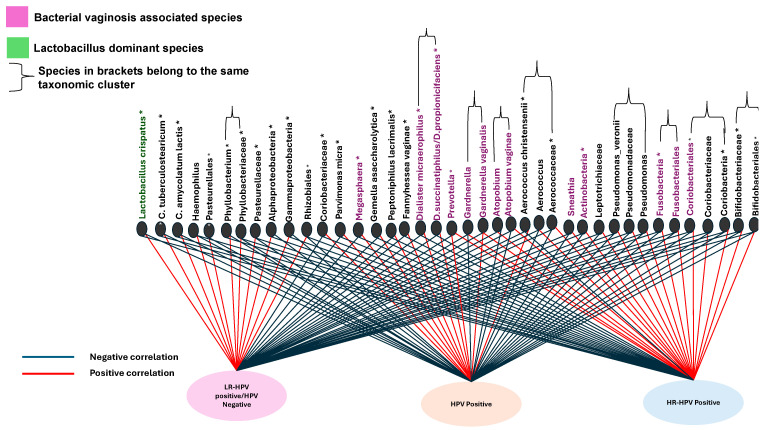
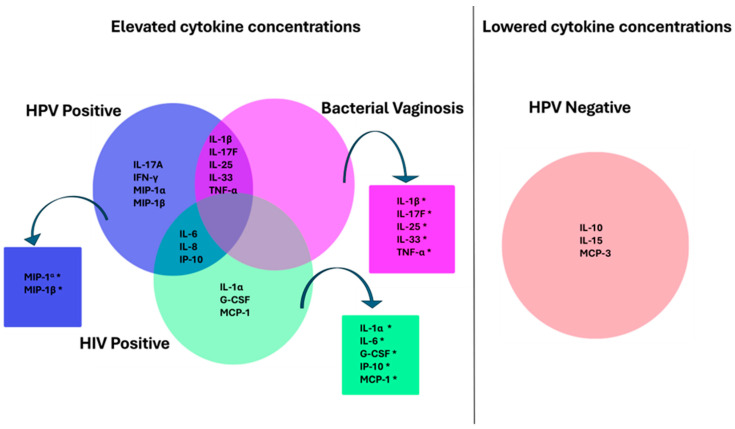
This systematic review and meta-analysis evaluate human papillomavirus (HPV) prevalence, genotype distribution, and associations with cervicovaginal microbiota and cytokine profiles among South African women, where cervical cancer ranks as the second most common cancer. PubMed, SCOPUS, and Web of Science were searched for studies on HPV infection up to 21 September 2024. The pooled prevalence was estimated using a random-effects model, with subgroup analyses by province, sample type, and HIV status. Publication bias was evaluated using funnel plots and Egger's test. Of the 19,765 studies screened, 120 met the inclusion criteria, comprising 83,266 participants. Results indicate a high HPV burden, with a pooled prevalence of 58% (95% CI: 52-64%), varying regionally from 53% (95% CI: 41-65%) to 64% (95% CI: 55-73%), with some regions under-researched. Cervical samples had the highest HPV prevalence (60% (95% CI: 54-66%)), while non-genital samples were less studied. High-risk (HR) HPV types, notably HPV 16 (7.5%), HPV 35 (4.1%), and HPV 18 (3.9%), were prominent, with HPV 35 emphasizing the need for expanded vaccine coverage. HIV-positive women had a higher pooled HPV prevalence (63% (95% CI: 55-71%)). Funnel plot analysis and Egger's test suggested a potential publication bias (p = 0.047). HPV-positive women exhibited lower Lactobacillus levels and an increase in Bacterial Vaginosis (BV)-associated species like Gardnerella, potentially supporting HPV persistence. Cytokine analysis showed elevated MIP-1α and MIP-1β in HPV infections, though cytokine profiles may depend on HPV genotypes. These findings underscore the need for research on HPV-microbiome-immune interactions and call for comprehensive HPV-prevention strategies, including vaccines targeting regional HPV types and tailored interventions for HIV-positive populations.
Keywords: cervical cancer; cervicovaginal microbiota; cytokines; genotype; human papillomavirus (HPV); prevalence.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Stuebs F.A., Gass P., Dietl A.K., Schulmeyer C.E., Adler W., Geppert C., Hartmann A., Knöll A., Beckmann M.W., Koch M.C. Human papilloma virus genotype distribution in women with premalignant or malignant lesions of the uterine cervix. Arch. Gynecol. Obstet. 2021;304:751–758. doi: 10.1007/s00404-021-05986-z. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
