

Inequities in the Use of Disease-Modifying Therapy Among Adults Living With Multiple Sclerosis in Urban and Rural Areas in Alberta, Canada
- PMID: 39772662
- PMCID: PMC11708828
- DOI: 10.1212/WNL.0000000000210251
Inequities in the Use of Disease-Modifying Therapy Among Adults Living With Multiple Sclerosis in Urban and Rural Areas in Alberta, Canada
Abstract
Objectives: To compare disease-modifying therapy (DMT) use between people living with multiple sclerosis (pwMS) who resided in rural vs urban areas.
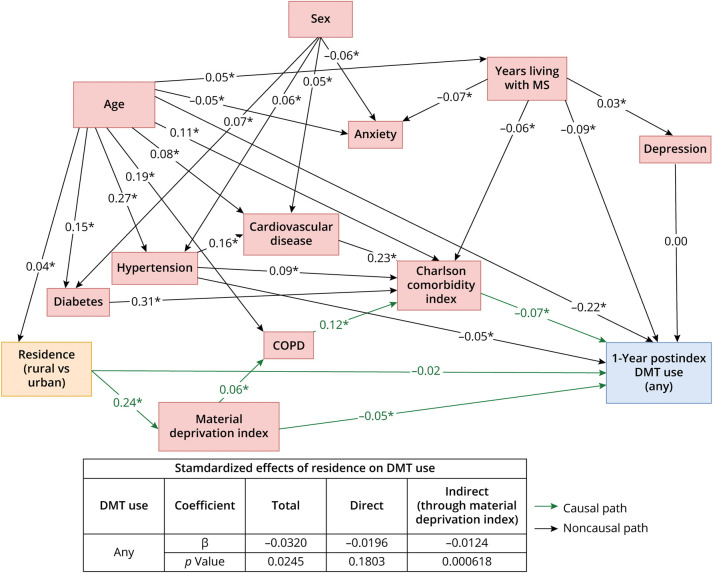
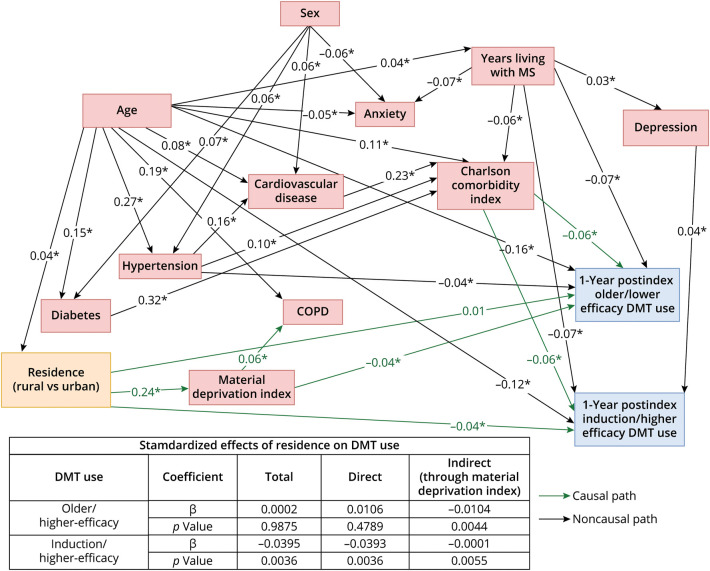
Methods: This retrospective cohort study used population-level individually linked administrative data to identify pwMS on April 1, 2019 (index date), in Alberta, Canada. DMT use was compared between pwMS who resided in rural vs urban areas during a 1-year postindex period. Structural equation modelling (SEM) and logistic regression (with 95% confidence intervals) were applied.
Results: PwMS (n = 4,593) who resided in rural areas (vs urban) were 17% less likely to have received a DMT (odds ratio: 0.83 [0.69-0.99]; SEM total β: -0.032, p < 0.05), of which 39% of this disparity was explained by a lower socioeconomic status (SEM indirect β: -0.012 [p < 0.001]/total β: -0.032); 26% were less likely to have received an induction/higher efficacy therapy (odds ratio: 0.74 [0.57-0.95]), of which <1% of this disparity was explained by socioeconomic status (SEM indirect β: -0.0001 [p < 0.01]/total β: -0.040).
Discussion: PwMS residing in rural (vs urban) Alberta are less likely to receive any DMT, especially induction/higher-efficacy therapy; this inequality may be mediated by socioeconomic status and geography. Identifying and overcoming barriers to optimal clinical care in this patient population is needed.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this manuscript: K. Vu, K.J.B. Martins, S. Aponte-Hao, L. Richer, T. Williamson, and S.W. Klarenbach are members of the Alberta Real World Evidence Consortium (ARWEC) and/or the Alberta Drug and Therapeutic Evaluation Consortium (ADTEC); these entities (composed of individuals from the University of Alberta, University of Calgary, and Institutes of Health Economics) conduct research including investigator-initiated industry-funded studies (ARWEC) and government-funded studies (ADTEC). E.F. Balcom, J.A. Mccombe, M.P. Kate, and P.S. Smyth declare no competing interests. All authors of this study had complete autonomy over the content and submission of the manuscript, as well as the design and execution of the study. Go to
Figures
References
-
- Spelman T, Magyari M, Piehl F, et al. Treatment escalation vs immediate initiation of highly effective treatment for patients with relapsing-remitting multiple sclerosis: data from 2 different national strategies. JAMA Neurol. 2021;78(10):1197-1204. doi: 10.1001/jamaneurol.2021.2738 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous